

Retrospective analysis of risk factors for stable chronic obstructive pulmonary disease combined with pulmonary hypertension
-
摘要:
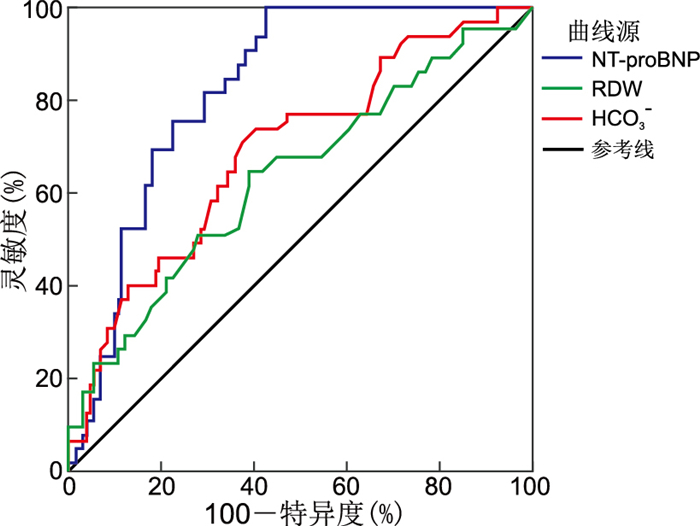
目的 分析稳定期慢性阻塞性肺疾病(COPD)合并肺动脉高压(PH)患者的临床特征和危险因素。 方法 选择2020年1月—2022年1月在宁夏医科大学总医院就诊的199例稳定期COPD合并PH患者和150例单纯稳定期COPD患者(作为对照组),比较2组患者的临床资料,并分析稳定期COPD合并不同严重程度PH的临床特征和危险因素。 结果 (1) COPD组与COPD合并PH组患者多个临床相关指标结果差异均有统计学意义。进一步将COPD合并PH患者分为轻度、中度和重度PH组,3组间红细胞分布宽度(RDW)、N末端B型脑钠肽原(NT-proBNP)、PCO2、HCO3-、每搏输出量(SV)和右室前后径(RVD)差异均有统计学意义(P < 0.05)。(2)相关性分析显示,心脏指数(CI)、系统免疫炎症指数(SII)和SV与肺动脉压力呈负相关,而RVD、RDW、PCO2、HCO3-、NT-proBNP与肺动脉压力均呈正相关关系。(3)多因素logistic回归分析结果显示,NT-proBNP值升高是稳定期COPD合并重度PH的独立危险因素(P < 0.05)。(4)ROC曲线结果显示,NT-proBNP的AUC值为0.827,高于RDW和HCO3-的AUC值。 结论 NT-proBNP值升高是稳定期COPD合并重度PH的独立危险因素;CI、SII、RDW、PCO2、HCO3-、NT-proBNP、SV和RVD与稳定期COPD合并PH具有相关性。 -
关键词:
- 稳定期慢性阻塞性肺疾病 /
- 肺动脉高压 /
- 危险因素
Abstract:Objective To analyze the clinical characteristics and risk factors of patients with stable chronic obstructive pulmonary disease (COPD) combined with pulmonary hypertension (PH). Methods A total of 199 patients with stable COPD combined with PH and 150 patients with pure stable COPD were collected from January 2020 to January 2022 at General Hospital of Ningxia Medical University as the control group. The clinical data of the two groups were compared, and the clinical characteristics and risk factors of stable COPD combined with different severity of PH were analyzed. Results (1) There were significant differences in several clinical indicators between the COPD group and the COPD combined with PH group. Furthermore, the COPD combined with PH patients were further divided into mild, moderate, and severe PH groups, and there were significant differences in red cell volume distribution width (RDW), N-terminal pro-brain natriuretic peptide (NT-proBNP), PCO2, HCO3-, stroke volume (SV), and right ventricular anterior-posterior diameter (RVD) among the three groups (P < 0.05). (2) Correlation analysis showed that cardiac index (CI), systemic immune-inflammation index (SII), and SV were negatively correlated with pulmonary artery pressure, while RDW, PCO2, HCO3-, and NT-proBNP were positively correlated with pulmonary artery pressure. (3) The results of multivariate logistic regression analysis showed that an elevated NT-proBNP level was an independent risk factor for severe PH in stable COPD (P < 0.05). (4) The ROC curve results showed that the AUC value of NT-proBNP was 0.827, higher than the AUC values of RDW and HCO3-. Conclusion An elevated NT-proBNP level is an independent risk factor for severe PH in stable COPD. In addition, there is a correlation between CI, SII, RDW, PCO2, HCO3-, NT-proBNP, SV, and RVD in stable COPD combined with PH. -

图 1 RDW、HCO3-和NT-proBNP对COPD合并重度PH预测价值的ROC曲线
Figure 1. ROC curves of the predictive value of RDW, HCO3-, and NT-proBNP for COPD combined with severe PH
表 1 COPD组和COPD组合并PH组患者各指标比较
Table 1. Comparison of the observation of various indicators in patients in COPD and COPD combined with PH group
项目 COPD
(n=150)COPD合并PH
(n=199)统计量 P值 年龄(x±s, 岁) 72.50±8.22 71.17±9.03 1.262a 0.194 性别(男性/女性,例) 91/59 114/85 -4.632b 0.367 BMI[M(P25, P75)] 21.76(20.03,24.22) 20.31(19.05,21.83) 0.735c 0.100 吸烟史(是/否,例) 98/52 123/76 -0.106b 0.325 WBC[M(P25, P75),×109/L] 7.74(5.97,9.89) 7.95(4.99,10.03) -0.841c 0.402 HGB(x±s,g/L) 159.09±17.60 157.43±19.85 1.697a 0.518 NEUT[M(P25, P75),×109/L] 5.70(4.38,7.30) 5.86(4.36,8.58) -0.207c 0.054 LYM(x±s,×109/L) 1.02±0.42 0.91±0.35 0.038a 0.013 PLT(x±s,×109/L) 203.53±65.03 192.08±48.85 2.376a 0.108 MPV(x±s,fL) 10.55±0.83 10.47±0.92 0.430a 0.086 RDW[M(P25, P75),%] 12.45(11.60,15.45) 14.50(13.50,17.60) -3.861c 0.024 NLR[M(P25, P75)] 4.23(2.27,7.25) 5.56(2.84,9.35) -1.870c 0.032 PLR[M(P25, P75)] 197.35(122.22,294.10) 203.69(120.40,307.60) -1.539c 0.296 SII[M(P25, P75)] 887.90(504.77,1 455.01) 1 024.33(507.29,2 812.09) -4.893c 0.015 NT-proBNP[M(P25, P75),pg/mL] 167.00(65.00,229.50) 745.00(288.00,1 560.00) -6.928c <0.001 Alb[M(P25, P75),g/L] 38.60(33.77,42.10) 36.53(34.60,40.00) 1.811c 0.012 D-二聚体[M(P25, P75),μg/mL] 0.59(0.37,1.21) 0.98(0.32,1.96) -3.225c 0.010 PH[M(P25, P75)] 7.40(7.37,7.41) 7.40(7.30,7.42) 0.110c 0.153 PCO2[M(P25, P75),mmHg] 43.90(40.05,50.80) 46.30(39.20,64.90) -2.378c 0.020 PO2[M(P25, P75),mmHg] 65.40(48.35,109.05) 66.90(46.80,110.20) -0.786c 0.064 Lac[M(P25, P75),mmol/L] 1.50(1.02,1.70) 1.70(1.45,5.40) -1.583c 0.045 HCO3-[M(P25, P75),mmol/L] 25.60(23.56,28.45) 28.50(26.40,34.20) -3.486c 0.003 SV(x±s,mL) 69.56±17.02 67.39±19.12 1.539a 0.031 MPAD[M(P25, P75),mm] 27.00(25.00,31.00) 29.00(27.25,34.55) -1.426c 0.021 LVDD(x±s,mm) 46.24±4.23 45.95±7.16 0.506a 0.145 RVD[M(P25, P75),mm] 21.00(20.00,22.00) 26.00(25.00,30.00) -4.751c <0.001 EF[M(P25, P75),%] 67.00(65.00,68.00) 66.98(62.54,69.78) 0.398c 0.287 CI(x±s) 3.38±0.91 3.03±0.94 1.384a 0.032 注:a为t值,b为χ2值, c为Z值。1 mmHg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 不同PH严重程度COPD患者临床指标比较
Table 2. Comparison of clinical indicators in COPD patients with different PH severity
项目 轻度PH(n=62) 中度PH(n=72) 重度PH(n=65) 统计量 P值 LYM(x±s, ×109/L) 1.11±0.63 0.96±0.45 1.00±0.51 0.749c 0.475 RDW[M(P25, P75),%] 13.35(12.50,14.80) 14.30(13.23,15.65) 14.60(13.40,17.00)a 8.566d 0.014 NLR[M(P25, P75)] 6.23(3.17,9.26) 5.12(2.69,9.43) 4.57(2.94,9.55) 0.302d 0.860 SII[M(P25, P75)] 1 065.67(605.54,2 115.01) 824.31(537.29,2 212.09) 902.83(507.49,1 732.20) 1.470d 0.242 NT-proBNP[M(P25, P75),pg/mL] 378.00(230.78,726.83) 649.80(453.18,1 290.00)a 880.90(1 170.00,1 420.00)ab 15.625d 0.012 Alb[M(P25, P75),g/L] 37.50(32.88,41.20) 34.90(32.10,37.93) 34.70(32.70,39.00) 2.797d 0.225 D-二聚体[M(P25, P75),μg/mL] 0.67(0.47,1.40) 1.06(0.59,2.22) 1.14(0.41,2.06) 2.772d 0.250 PCO2[M(P25, P75),mmHg] 40.90(37.05,46.80) 43.25(37.48,56.75) 48.30(41.80,63.90)a 8.007d 0.028 Lac[M(P25, P75),mmHg] 1.33(1.02,1.70) 1.27(0.87,2.02) 3.20(1.45,6.50) 0.050d 0.975 HCO3-[M(P25, P75),mmol/L] 25.00(23.56,28.45) 27.35(23.30,31.88)a 29.40(26.40,34.20)ab 10.390d 0.006 SV(x±s,mL) 72.04±17.46 62.18±13.31a 55.13±19.39a 8.632c <0.001 MPAD[M(P25, P75),mm] 28.00(26.25,30.75) 29.00(28.00,31.00) 30.00(28.00,34.00) 3.006d 0.223 RVD[M(P25, P75),mm] 24.00(19.00,28.75) 25.00(22.00,27.25) 30.00(27.00,35.00)ab 20.079d <0.001 CI(x±s) 3.35±0.96 3.14±1.16 2.73±0.96 6.619c 0.002 注:与轻度组比较,aP < 0.05;与中度组比较,bP < 0.05。c为F值,d为H值。
下载: 导出CSV
表 3 各指标与肺动脉压力的相关性
Table 3. Correlation between various index and pulmonary artery pressure
项目 r值 P值 CI -0.324 0.001 SV -0.463 < 0.001 RVD 0.328 0.001 RDW 0.261 0.006 PCO2 0.207 0.031 HCO3- 0.324 0.001 SII -0.122 0.046 NLR 0.082 0.394 PLR 0.052 0.589 NT-proBNP 0.442 0.001
下载: 导出CSV
表 4 变量赋值方法
Table 4. Variable assignment method
变量 赋值方法 性别 男性=1,女性=2 吸烟史 否=0,是=1 COPD合并重度PH 否=0,是=1 连续变量 以实际值赋值
下载: 导出CSV
表 5 COPD合并重度PH影响因素的单因素logistic回归分析
Table 5. Univariate logistic regression analysis of the influencing factors of COPD combined with severe PH
因素 B SE Waldχ2 P值 OR值 95% CI RDW 0.187 0.078 5.763 0.016 1.206 1.035~1.405 HCO3- 0.125 0.043 8.357 0.004 1.133 1.041~1.234 PCO2 0.023 0.014 2.443 0.118 1.023 0.994~1.052 NT-proBNP 0.002 0.001 9.522 0.020 1.002 1.001~1.004 SII -0.002 0.011 0.031 0.861 0.998 0.978~1.019
下载: 导出CSV
表 6 COPD合并重度PH影响因素的多因素logistic回归分析
Table 6. Multivariate logistic regression analysis of the influencing factors of COPD combined with severe PH
变量 B SE Waldχ2 P值 OR值 95% CI RDW 0.384 0.330 1.359 0.244 1.469 0.770~2.830 HCO3- 0.393 0.238 2.717 0.099 1.481 0.928~2.362 NT-proBNP 0.003 0.001 10.041 0.020 1.003 1.001~1.004
下载: 导出CSV
-
[1] Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2021 REPORT)[EB/OL]. (2021-11-18)[2023-05-12]. https://goldcopd.org/goldreports/ .[2] 中华医学会呼吸病学分会肺栓塞与肺血管病学组, 中国医师协会呼吸医师分会肺栓塞与肺血管病工作委员会, 全国肺栓塞与肺血管病防治协作组, 等. 中国肺动脉高压诊断与治疗指南(2021版)[J]. 中华医学杂志, 2021, 101(1): 11-51. https://www.cnki.com.cn/Article/CJFDTOTAL-QKYX202303020.htmPulmonary Embolism and Pulmonary Vascular Disease Group of the Respiratory Disease Branch of the Chinese Medical Association, Pulmonary Embolism and Pulmonary Vascular Disease Working Committee of the Respiratory Physicians 'Branch of the Chinese Physicians' Association, and National Collaborative Group for the Prevention and Treatment of Pulmonary Embolism and Pulmonary Vascular Disease, et al. Chinese guidelines for the diagnosis and treatment of pulmonary hypertension (2021 edition)[J]. National Medical Journal of China, 2021, 101(1): 11-51. https://www.cnki.com.cn/Article/CJFDTOTAL-QKYX202303020.htm [3] ZHONG Y, YU P B. Decoding the link between inflammation and pulmonary arterial hypertension[J]. Circulation, 2022, 146(13): 1023-1025. doi: 10.1161/CIRCULATIONAHA.122.059949 [4] HUMBERT M, KOVACS G, HOEPER M M, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension[J]. Eur Heart J, 2022, 43(38): 3618-3731. doi: 10.1093/eurheartj/ehac237 [5] KADER M N, MOIZ J A, BHATI P, et al. Diagnostic validity of cardiopulmonary exercise testing for screening pulmonary hypertension in patients with chronic obstructive pulmonary disease[J]. J Cardiopulm Rehabil Prev, 2020, 40(3): 189-194. doi: 10.1097/HCR.0000000000000456 [6] JIANG T T, WANG Q, ZHANG Z P, et al. Value of the neutrophil-to-lymphocyte ratio in chronic obstructive pulmonary disease complicated with pulmonary hypertension[J]. J Int Med Res, 2023, 51(9): 3000605231200266. DOI: 10.1177/03000605231200266. [7] WANG C, XU J Y, YANG L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health[CPH] study): a national cross-sectional study[J]. Lancet, 2018, 391(10131): 1706-1717. doi: 10.1016/S0140-6736(18)30841-9 [8] NATHAN S D, BARBERA J A, GAINE S P, et al. Pulmonary hypertension in chronic lung disease and hypoxia[J]. Eur Respir J, 2019, 53(1): 1801914. DOI: 10.1183/13993003.01914-2018. [9] GREDIC M, BLANCO I, KOVACS G, et al. Pulmonary hypertension in chronic obstructive pulmonary disease[J]. Br J Pharmacol, 2021, 178(1): 132-151. doi: 10.1111/bph.14979 [10] VERGARO G, AIMO A, JANUZZI J L, et al. Cardiac biomarkers retain prognostic significance in patients with heart failure and chronic obstructive pulmonary disease[J]. J Cardiovasc Med (Hagerstown), 2022, 23(1): 28-36. doi: 10.2459/JCM.0000000000001281 [11] ERMINI L, SEDDONE S, POLICASTRO P, et al. The cardiac caval index: improving noninvasive assessment of cardiac preload[J]. J Ultrasound Med, 2022, 41(9): 2247-2258. doi: 10.1002/jum.15909 [12] 魏瑞奇, 朴春梅, 张文美, 等. 血小板在肺动脉高压发生、发展中的作用[J]. 国际呼吸杂志, 2020, 40(10): 790-795.WEI R Q, PU C M, ZHANG W M, et al. The role of platelets in the development and progression of pulmonary hypertension[J]. International Respiratory Journal, 2020, 40(10): 790-795. [13] KAZIMIERCZYK R, KAMIŃSKI K. The role of platelets in the development and progression of pulmonary arterial hypertension[J]. Adv Med Sci, 2018, 63(2): 312-316. doi: 10.1016/j.advms.2018.04.013 [14] GALLARDO-VARA E, NTOKOU A, DAVE J M, et al. Vascular pathobiology of pulmonary hypertension[J]. J Heart Lung Transplant, 2023, 42(5): 544-552. doi: 10.1016/j.healun.2022.12.012 [15] ZHU Y, SHU D, GONG X, et al. Platelet-Derived TGF (Transforming Growth Factor)-β1 enhances the aerobic glycolysis of pulmonary arterial smooth muscle cells by PKM2 (Pyruvate Kinase Muscle Isoform 2) upregulation[J]. Hypertension, 2022, 79(5): 932-945. doi: 10.1161/HYPERTENSIONAHA.121.18684 [16] BALTAZARES-LIPP M E, AGUILERA-VELASCO A, AQUINO-GÁLVEZ A, et al. Evaluating of red blood cell distribution width, comorbidities and electrocardiographic ratios as predictors of prognosis in patients with pulmonary hypertension[J]. Diagnostics (Basel), 2021, 11(7): 1297. doi: 10.3390/diagnostics11071297 [17] VITKAUSKAITE A, URBONIENE D, CELIESIUTE J, et al. Circulating inflammatory markers in cervical cancer patients and healthy controls[J]. J Immunotoxicol, 2020, 17(1): 105-109. doi: 10.1080/1547691X.2020.1755397 [18] 朱悦, 孙耕耘. 中性粒细胞/淋巴细胞比值及血小板相关指标与OSAS患者严重程度的相关性研究[J]. 中华全科医学, 2019, 17(3): 347-350, 474. doi: 10.16766/j.cnki.issn.1674-4152.000678ZHU Y, SUN G Y. NLR, PLR and MPV related to the severity of obstructive sleep apnea syndrome[J]. Chinese Journal of General Practice, 2019, 17(3): 347-350, 474. doi: 10.16766/j.cnki.issn.1674-4152.000678 [19] SHAHMORADI Z, MALEKMOHAMMAD M, NAJAFI G, et al. Prognostic value of platelet to lymphocyte ratio (PLR) and neutrophil to lymphocyte ratio (NLR) in patients with pulmonary hypertension[J]. Tanaffos, 2022, 21(4): 480-486. [20] TIAN B W, YANG Y F, YANG C C, et al. Systemic immune-inflammation index predicts prognosis of cancer immunotherapy: systemic review and meta-analysis[J]. Immunotherapy, 2022, 14(18): 1481-1496. doi: 10.2217/imt-2022-0133 [21] ZUO H H, XIE X C, PENG J H, et al. Predictive value of novel inflammation-based biomarkers for pulmonary hypertension in the acute exacerbation of chronic obstructive pulmonary disease[J]. Anal Cell Pathol (Amst), 2019: 5189165. DOI: 10.1155/2019/5189165. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 359
- HTML全文浏览量: 157
- PDF下载量: 27
- 被引次数: 0
