

Etiological characteristics of recurrent urinary tract infection in children and construction of risk factors model for recurrence
-
摘要:
目的 探究小儿再发性尿路感染的病原学特征,以期为临床早期识别高危患儿及制定个体化干预策略提供参考。 方法 选取2021年7月—2024年12月首都儿科研究所附属儿童医院收治的160例尿路感染患儿,收集患儿的一般资料、临床症状,并随访半年,根据患儿尿路感染再发情况分为非再发组103例和再发组57例。比较2组患儿尿路感染临床特征,采用logistic回归分析筛选预测变量并建立预测模型。 结果 选取160例患儿首次感染时共培养出的病原菌175株,以大肠埃希菌感染为主。再发组患儿大肠埃希菌感染占比高于非再发组,复杂性感染占比高于非再发组(P<0.05)。再发组贫血、泌尿系统畸形、留置导尿时间为5~10 d及IgA水平降低的患儿占比均高于非再发组(P<0.05)。Logistic多因素分析结果显示,复杂性感染、泌尿系统畸形、未规范使用抗生素均是导致小儿尿路感染再发的独立危险因素(P < 0.05)。模型验证结果显示,AUC为0.773(95% CI:0.684~0.862),提示该模型区分度较好;校准曲线与理想曲线较为接近(Hosmer-Lemeshow P=0.152),表明该模型具有良好的预测效能;决策曲线显示,当预测概率阈值在0.10~0.97的范围内使用本研究模型具有较高的预测净获益值。 结论 小儿再发性尿路感染主要病原体为大肠埃希菌,以复杂性感染为主。复杂性感染、泌尿系统畸形及未规范使用抗生素是再发感染的独立危险因素,早期识别与干预有助于改善预后。 Abstract:Objective To explore the etiological characteristics of recurrent urinary tract infection in children, aiming to provide a reference for the early clinical identification of high-risk children and the formulation of individualized intervention strategies. Methods A total of 160 children with urinary tract infection in the Children's Hospital Affiliated to Capital Institute of Pediatrics were selected from July 2021 to December 2024. The general data and clinical symptoms of children were collected. The patients were followed up for half a year and divided into non-recurrence group (103 cases) and recurrence group (57 cases) based on the recurrence status of urinary tract infection. The two groups were compared in terms of differences in clinical characteristics of urinary tract infection. Logistic regression analysis was performed to screen the predictive variables, and a prediction model was established. Results A total of 175 strains of pathogenic bacteria were cultured in 160 children with first infection, with Escherichia coli being the predominant pathogen. The rate of Escherichia coli infection in the recurrent children was higher than that in the non-recurrent children, and the rate of complex infection was also higher (P < 0.05). The recurrence group exhibited higher proportions of children with anemia, urinary system malformation, indwelling catheterization time of 5-10 d and reduced IgA than the non-recurrence group (P < 0.05). Multivariate analysis suggested that complex infection, urinary system malformation, and non-standard use of antibiotics were independent risk factors of recurrence of urinary tract infection in children (P < 0.05). The results of model validation showed that AUC was 0.773 (95% CI: 0.684-0.862), indicating that the model had a good discrimination degree. The calibration curve was close to the ideal curve (Hosmer-Lemeshow P=0.152), indicating that the model had good predictive efficiency. Decision curve revealed that when the prediction probability threshold was in the range of 0.10-0.97, the model of this study had a higher predicted net benefit value. Conclusion The main pathogen of recurrent urinary tract infection in children is Escherichia coli, and complex infection is predominant. Complex urinary tract infection, urinary system malformation and non-standard use of antibiotics are independent risk factors of recurrence. Early identification and intervention can help to improve the prognosis. -
Key words:
- Urinary tract infection /
- Children /
- Etiological characteristics /
- Risk of recurrence
-

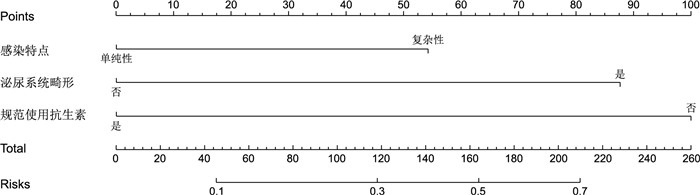
图 1 基于多因素分析的小儿尿路感染再发风险预测列线图模型
Figure 1. Risk prediction nomogram model for recurrence of urinary tract infection in children
表 1 再发组和非再发组尿路感染患儿的病原菌分布情况[株(%)]
Table 1. Distribution of pathogenic bacteria in children with recurrent and non-recurrent urinary tract infections
组别 株数 大肠埃希菌 肺炎克雷伯菌 粪肠球菌 金黄色葡萄球菌 其他 非再发组 114 68(59.6) 21(18.4) 9(7.9) 11(9.7) 5(4.4) 再发组 61 23(37.7) 15(24.6) 9(14.8) 9(14.8) 5(8.2) χ2值 7.666 0.926 2.026 1.023 1.071 P值 0.006 0.336 0.115 0.312 0.301  下载: 导出CSV
下载: 导出CSV
表 2 再发组和非再发组尿路感染患儿临床症状比较[例(%)]
Table 2. Comparison of clinical symptoms between children with recurrent urinary tract infection and non-recurrent urinary tract infection
组别 例数 乏力 尿膀胱刺激征阳性 排尿困难 脓尿 血尿 蛋白尿 尿色浑浊 肾区叩痛 腹痛 腹泻 便血 头晕头痛 非再发组 103 92(89.3) 43(41.7) 18(17.5) 12(11.7) 9(8.7) 11(10.7) 22(21.4) 8(7.8) 10(9.7) 9(8.7) 6(5.8) 65(63.1) 再发组 57 46(80.7) 32(56.1) 15(26.3) 13(22.8) 6(10.5) 8(14.0) 15(26.3) 7(12.3) 8(14.0) 8(14.0) 5(8.8) 41(71.9) χ2值 2.298 3.052 1.752 3.464 0.138 0.395 0.507 0.880 0.688 1.084 0.498 1.278 P值 0.130 0.081 0.186 0.063 0.710 0.395 0.476 0.348 0.407 0.298 0.481 1.560
下载: 导出CSV
表 3 再发组和非再发组尿路感染患儿的临床资料比较
Table 3. Comparison of clinical data of children with urinary tract infection in relapse group and non-relapse group
组别 例数 性别
(男/女,例)年龄≤3岁
[例(%)]过敏体质
[例(%)]贫血
[例(%)]便秘
[例(%)]泌尿系统畸
形[例(%)]住院时间
(< 15 d/≥15 d,例)留置导尿时间
(<5 d/5~10 d,例)膀胱类型(尿潴留
/尿失禁/混合型,例)IgA水平降低
[例(%)]IgG水平降低
[例(%)]规范使用抗生
素[例(%)]非再发组 103 56/47 43(41.7) 43(41.7) 51(49.5) 53(51.5) 31(30.1) 36/67 67/36 26/24/53 51(49.5) 49(47.6) 47(45.6) 再发组 57 23/34 29(50.9) 31(54.4) 44(77.2) 32(56.1) 35(61.4) 15/42 21/36 19/15/23 39(68.4) 31(54.4) 12(21.1) χ2值 2.885 1.236 2.358 11.654 0.323 14.840 1.260 11.795 1.944 5.330 0.681 9.523 P值 0.089 0.266 0.125 0.001 0.570 < 0.001 0.262 0.001 0.378 0.021 0.409 0.002
下载: 导出CSV
表 4 小儿尿路感染再发风险的单因素logistic回归分析
Table 4. Univariate logistic regression analysis of urinary tract infection recurrence in children
自变量 B SE Waldχ2 P值 OR值 95%CI 感染特点 0.828 0.401 4.264 0.039 2.288 1.042~5.023 贫血 0.862 0.417 2.368 0.039 2.368 1.046~5.359 泌尿系统畸形 1.252 0.407 3.497 0.002 3.496 1.574~7.764 留置导尿时间 0.832 0.397 4.392 0.036 2.297 1.056~4.997 IgA水平降低 0.865 0.410 4.451 0.035 2.376 1.063~5.308 规范使用抗生素情况 1.551 0.478 10.529 0.001 4.714 1.847~12.036
下载: 导出CSV
表 5 小儿尿路感染再发风险的多因素logistic回归分析
Table 5. Multivariate logistic regression analysis of urinary tract infection recurrence in children
自变量 B SE Waldχ2 P值 OR值 95%CI 感染特点 1.126 0.506 4.952 0.026 3.083 1.144~8.313 贫血 0.906 0.601 2.273 0.132 2.474 0.762~8.030 泌尿系统畸形 1.447 0.573 6.377 0.012 4.248 1.381~13.069 留置导尿时间5~10 d 0.401 0.530 0.572 0.449 1.493 0.529~4.215 IgA水平降低 0.662 0.529 1.566 0.211 1.939 0.687~5.468 规范使用抗生素情况 1.708 0.573 8.885 0.003 5.517 1.796~16.950
下载: 导出CSV
-
[1] BRANDSTROM P, HANSSON S. Urinary tract infection in children[J]. Pediatr Clin North Am, 2022, 69(6): 11099-1114. [2] YANG S S, TSAI J D, KANEMATSU A, et al. Asian guidelines for urinary tract infection in children[J]. J Infect Chemother, 2021, 27(11): 1543-1554. doi: 10.1016/j.jiac.2021.07.014 [3] 吴瑞萍, 胡亚美, 江载芳. 实用儿科学(下册)[M]. 6版. 北京: 人民卫生出版社, 1996: 296.WU R P, HU Y M, JIANG Z F. Applied Pediatrics[M]. 6th Ed (Volume 2). Beijing: People' s Medical Publishing House, 1996: 296. [4] 王海燕. 肾脏病学[M]. 2版. 北京: 人民卫生出版社, 1996: 811-821.WANG H Y. Nephrology[M]. 2nd Ed. Beijing: People' s Medical Publishing House, 1996: 811-821. [5] 周广伦, 孙俊杰, 尹鉴淳, 等. 儿童神经源性膀胱并尿路感染的临床特点及病原菌分析[J]. 临床小儿外科杂志, 2021, 20(11): 1021-1025.ZHOU G L, SUN J J, YIN J C, et al. Analysis of pathogens and clinical features of neuropathic bladder with urinary tract infection in children[J]. Journal of Clinical Pediatric Surgery, 2021, 20(11): 1021-1025. [6] 尼加提·阿力木, 马士凤, 夏木斯娅·阿里木江, 等. 儿童糖尿病合并尿路感染的临床特征及危险因素分析[J]. 天津医药, 2024, 52(10): 1051-1055.NIJAT·ALM, MA S F, XAMSIYA·ALMJ, et al. Analysis of clinical characteristics and risk factors for diabetes mellitus complicated with urinary tract infection in children[J]. Tianjin Medical Journal, 2024, 52(10): 1051-1055. [7] 孙金山, 陈朝英. 儿童复杂性泌尿道感染临床表现和预后分析[J]. 临床儿科杂志, 2021, 39(2): 102-107.SUN J S, CHEN C Y. Clinical features and prognostic analysis of complicated urinary tract infection in children[J]. Journal of Clinical Pediatrics, 2021, 39(2): 102-107. [8] 吴文华, 张芷铭. 儿童复杂性泌尿道感染症状及预后的临床分析[J]. 世界最新医学信息文摘, 2022, 22(54): 13-16.WU W H, ZHANG Z M. Clinical analysis of symptoms and prognosis of complicated urinary tract infections in children[J]. World Latest Medicine Information, 2022, 22(54): 13-16. [9] 韩艳超, 杨文静. 小儿尿路感染的临床特点及其影响因素分析[J]. 安徽医学, 2020, 41(12): 1451-1454.HAN Y C, YANG W J. Clinical characteristics and influencing factors of urinary tract infection in children[J]. Anhui Medical Journal, 2020, 41(12): 1451-1454. [10] 梁樱凡, 陈星意, 李玲. 老年患者真菌性尿路感染临床特点及危险因素分析[J]. 中国真菌学杂志, 2024, 19(4): 385-388.LIANG Y F, CHEN X Y, LI L. Analysis of clinical characteristics and risk factors of fungal urinary tract infection in elderly patients[J]. Chinese Journal of Mycology, 2024, 19(4): 385-388. [11] 孙婕, 孙宁, 张潍平, 等. 输尿管远端直径比对儿童原发性膀胱输尿管反流早期突破性尿路感染的预测作用研究[J]. 临床小儿外科杂志, 2023, 22(10): 917-923.SUN J, SUN N, ZHANG W P, et al. Role of distal ureteral diameter ratio in predicting early breakthrough urinary tract infections in children with primary vesicoureteral reflux[J]. Journal of Clinical Pediatric Surgery, 2023, 22(10): 917-923. [12] 黄海林, 梁勇升, 唐培佳, 等. 快速康复外科理念麻醉管理在小儿先天性心脏病经胸介入手术治疗中的作用及安全性[J]. 中国临床研究, 2021, 34(4): 482-485.HUANG H L, LIANG Y S, TANG P J, et al. Effect and safety of "enhanced recovery after surgery" anesthesia management on children with congenital heart disease treated by transthoracic interventional surgery[J]. Chinese Journal of Clinical Research, 2021, 34(4): 482-485. [13] 陈怡, 陈沛林, 吕晓磊, 等. 膀胱癌尿路感染患者免疫和炎症因子的表达及临床诊断价值[J]. 中华医院感染学杂志, 2022, 32(1): 80-84.CHEN Y, CHEN P L, LYU X L, et al. Expression of immune and inflammatory factors in bladder cancer patients with urinary tract infection and clinical diagnostic values[J]. Chinese Journal of Nosocomiology, 2022, 32(1): 80-84. [14] 刘鑫, 刘舸, 杨屹. 儿童原发性膀胱输尿管反流突破性尿路感染的风险因素分析[J]. 临床小儿外科杂志, 2023, 22(10): 911-916.LIU X, LIU G, YANG Y. Related factors predicting breakthrough febrile urinary tract infection in children with vesicoureteral reflux[J]. Journal of Clinical Pediatric Surgery, 2023, 22(10): 911-916. [15] 吉潘阿呷木, 周太光. 儿童泌尿道感染591例临床特点及病原菌分析[J]. 微生物与感染, 2023, 18(2): 83-90.JIPAN AGM, ZHOU T G. Clinical characteristics and pathogens analysis of 591 children with urinary tract infection[J]. Journal of Microbes and Infections, 2023, 18(2): 83-90. [16] 孙金山, 陈朝英, 涂娟, 等. 2018—2023年北京地区单中心儿童泌尿道感染病原菌分布和耐药率分析[J]. 中华肾脏病杂志, 2024, 40(12): 940-945.SUN J S, CHEN C Y, TU J, et al. Pathogenic bacteria distribution and antimicrobial resistance in children with urinary tract infection in a single center in Beijing[J]. Chinese Journal of Nephrology, 2024, 40(12): 940-945. [17] 赵盈盈, 李爽, 张鑫, 等. 上尿路梗阻患者术后感染及应对方式与生活质量的相关性[J]. 中华全科医学, 2025, 23(8): 1411-1414. doi: 10.16766/j.cnki.issn.1674-4152.004145ZHAO Y Y, LI S, ZHANG X, et al. The correlation among postoperative infection, coping modes, and quality of life in patients with urinary tract obstruction[J]. Chinese Journal of General Practice, 2025, 23(8): 1411-1414. doi: 10.16766/j.cnki.issn.1674-4152.004145 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 13
- HTML全文浏览量: 7
- PDF下载量: 1
- 被引次数: 0
