

Investigation into the use of an intelligent follow-up management system for enhancing self-management skills in patients with chronic kidney disease
-
摘要:
目的 将智能随访管理系统应用于慢性肾脏病患者中,评估其对患者自我管理能力的影响。 方法 选取2022年4月—2023年3月宁波大学附属第一医院的207例慢性肾脏病患者,采用随机数字表法分为干预组(103例)和对照组(104例)。对照组采用常规随访,干预组采用智能随访。干预前、干预6个月、12个月后,比较2组的自我管理能力、生理指标、规范随访率及非计划住院率情况。 结果 干预6个月、12个月后干预组自我管理能力总分为(82.49±6.58)分和(89.07±5.29)分,高于对照组的(77.25±10.56)分和(78.41±9.24)分,差异均有统计学意义(P<0.001);干预组健康指标[估算肾小球滤过率差值(ΔeGFR)、BMI达标率、舒张压、收缩压]优于对照组,差异均有统计学意义(P<0.05)。干预后,干预组规范随访率为86.80%(80.00%, 100.00%),高于对照组的71.15%(50.00%, 100.00%),差异有统计学意义(Z=5.241,P<0.001);干预组非计划住院率为15.5%(15/97), 低于对照组的28.0%(28/100),差异有统计学意义(χ2=4.535,P=0.033)。 结论 智能随访管理系统能提高慢性肾脏病患者的自我管理能力,改善健康指标。 -
关键词:
- 信息-动机-行为技巧模型 /
- 慢性肾脏病 /
- 智能随访 /
- 自我管理 /
Abstract:Objective The intelligent follow-up management system was applied in patients with CKD to evaluate its effects on self-management ability. Methods From April 2022 to March 2023, 207 patients with CKD recruited from a tertiary hospital in Zhejiang Province were randomly allocated into an intervention group (n=103) and a control group (n=104). The control group was followed up regularly, while the intervention group adopted intelligent follow-up management. Self-management ability, physiological indicators, standardized follow-up rate, and unplanned hospitalization rate were compared between the two groups before the intervention, 6 months post-intervention, and 12 months post-intervention. Results At 6 months and 12 months post-intervention, the intervention group's total self-management ability scores were (82.49±6.58) points and (89.07±5.29) points, respectively, which were significantly higher than those of the control group (77.25±10.56) points and (78.41±9.24)points, with statistically significant differences (P < 0.001); health indicators of the intervention group, including the estimated glomerular filtration rate difference (ΔeGFR), BMI compliance rate, diastolic blood pressure and systolic blood pressure were superior to those of the control group, with statistically significant differences (P < 0.05). After the intervention, the intervention group achieved a significantly higher standardized follow-up rate [86.80% (80.00%, 100.00%)] compared to the control group [71.15% (50.00%, 100.00%), Z=5.241, P < 0.001]; clinically meaningful reductions in unplanned hospitalization rate were achieved in the intervention group 15.5% (15/97), substantially below control levels 28.0% (28/100), with statistical confirmation (χ2=4.535, P=0.033). Conclusion The intelligent follow-up management system can significantly enhance self-management proficiency in patients with CKD, improve health indicators. -

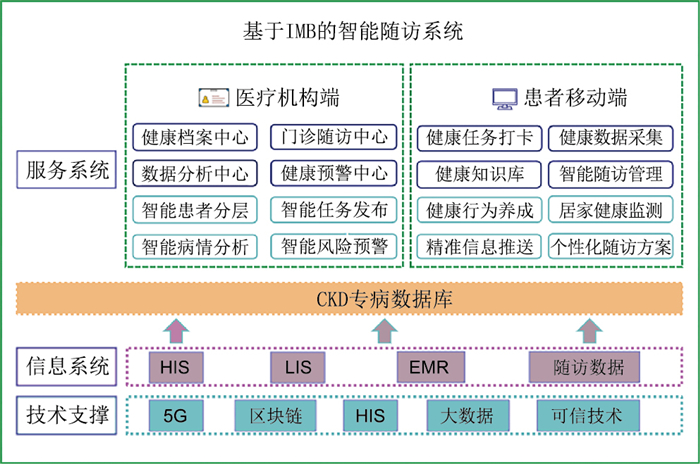
图 1 基于IMB的智能随访系统功能模块
Figure 1. Functional modules of IMB-based intelligent follow-up system
表 1 2组慢性肾脏病患者基本资料比较
Table 1. Comparison of baseline data between two groups of CKD patients
项目 干预组(n=97) 对照组(n=100) 统计量 P值 年龄(x±s,岁) 51.76±12.89 48.63±10.21 1.890a 0.060 性别[例(%)] 0.141b 0.707 男性 54(55.7) 53(53.0) 女性 43(44.3) 47(47.0) 文化程度[例(%)] -1.241c 0.215 小学及以下 34(35.1) 28(28.0) 初中 31(31.9) 36(36.0) 高中 20(20.6) 13(13.0) 大学 12(12.4) 23(23.0) 婚姻状况[例(%)] 0.544b 0.910 已婚 90(92.8) 93(93.0) 未婚 6(6.2) 5(5.0) 离异 1(1.0) 2(2.0) 病程[M(P25, P75),年] 2.0(1.0, 4.0) 2.0(1.0, 5.0) -0.835c 0.404 分期[例(%)] -2.698c 0.072 CKD2期 49(50.5) 50(50.0) CKD3A期 16(16.5) 21(21.0) CKD3B期 14(14.4) 13(13.0) CKD4期 18(18.6) 16(16.0) 支付方式[例(%)] 0.021b 0.885 医保 86(88.7) 88(88.0) 自费 11(11.3) 12(12.0) eGFR(x±s,μmol/L) 41.60±1.66 37.90±1.55 1.350a 0.098 收缩压(x±s,mmHg) 132.31±16.61 129.01±9.95 1.685a 0.094 舒张压(x±s,mmHg) 82.60±12.14 80.22±7.43 1.653a 0.100 BMI(x±s) 23.82±3.49 23.43±2.99 0.856a 0.393 注:a为t值,b为χ2值,c为Z值。1 mmHg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 基于IMB模型的智能随访干预方案
Table 2. Intelligent follow-up intervention plan based on the IMB model
干预主题 类别 干预内容 信息干预 智能健康宣教 智能精准推送宣教内容、查阅患者学习状态,未完成者再次发送提醒,定期评估知识掌握度 线上互动问答 患者发起线上问诊,随访团队及时解答 动机干预 个人动机干预 了解患者心理需求,疏导负性情绪;了解患者对健康生活方式的态度和信念,对治疗的顾虑,针对不遵医的态度和行为给予干预 社会动机干预 邀请家属参与诊疗及健康教育,建立患者社会支持网络,协助其行为改变 行为技巧干预 肾康复方案 医患协同制定治疗方案,包括疾病控制、运动、饮食等 智能食谱制定 系统智能生成一周食谱,患者记录饮食日记并上传,由营养师评价并调整 智能预警 实时分析患者生理指标,智能预警,CKD管理护士持续跟进 智能复诊提醒 提前15 d复诊提醒,未复诊患者执行主动追踪 智能健康报告 每月生成病情报告,供CKD团队评估,对存在问题进行追踪,形成闭环管理
下载: 导出CSV
表 3 2组CKD患者干预前后自我管理能力比较(x±s, 分)
Table 3. A comparative of the variations in self-management abilities pre- and post-intervention among two groups of CKD patients (x±s, points)
组别 例数 干预前 干预后6个月 干预后12个月 F值 P值 对照组 100 77.53±8.90 77.25±10.56 78.41±9.24 0.472 0.624 干预组 97 76.74±8.02 82.49±6.58a 89.07±5.29ab 81.711 <0.001 F值 0.523 18.100 98.170 P值 0.471 <0.001 <0.001 注:与同组干预前比较,aP<0.05;与同组干预6个月比较,bP<0.05。
下载: 导出CSV
表 4 2组CKD患者干预后ΔeGFR比较(x±s, μmol/L)
Table 4. A comparative of the variations in ΔeGFR after intervention among two groups of CKD patients
组别 例数 6个月—干预前 12个月—干预前 t值 P值 对照组 100 0.19±8.46 -3.69±9.06 3.137 0.002 干预组 97 2.67±8.00 4.55±9.03 1.540 0.125 统计量 2.106a 39.594b P值 0.037 <0.001 注:a为t值,b为F值。
下载: 导出CSV
表 5 2组CKD患者干预前后收缩压比较(x±s,mmHg)
Table 5. A comparative of the variations in systolic blood pressure pre- and post-intervention among two groups of CKD patients
组别 例数 干预前 干预后6个月 干预后12个月 F值 P值 对照组 100 129.01±9.95 130.11±10.15 132.49±13.04a 2.551 0.108 干预组 97 132.31±16.61 122.15±13.75a 118.82±11.20a 24.319 <0.001 F值 2.880 21.443 62.069 P值 0.094 <0.001 <0.001 注:与同组干预前比较,aP<0.05。
下载: 导出CSV
表 6 2组CKD患者干预前后舒张压比较(x±s, mmHg)
Table 6. A comparative of the variations in diastolic blood pressure pre- and post-intervention among two groups of CKD patients
组别 例数 干预前 干预后6个月 干预后12个月 F值 P值 对照组 100 80.22±7.43 79.61±8.11 84.13±10.70ab 7.668 0.002 干预组 97 82.60±12.14 75.41±9.42a 74.00±7.63a 21.026 <0.001 F值 2.770 11.257 58.262 P值 0.100 0.001 <0.001 注:与同组干预前比较,aP<0.05;与同组干预6个月比较,bP<0.05。
下载: 导出CSV
表 7 2组CKD患者干预前后BMI达标率比较[例(%)]
Table 7. A comparative of BMI compliance rate pre- and post-intervention among two groups of patients with CKD
组别 例数 干预前 干预后6个月 干预后12个月 χ2值 P值 对照组 100 39(39.0) 40(40.0) 47(47.0) 1.560 0.458 干预组 97 42(43.3) 50(51.5) 60(61.9)a 6.721 0.035 χ2值 0.376 2.645 4.479 P值 0.540 0.104 0.036 注:与同组干预前比较,aP<0.05。
下载: 导出CSV
表 8 2组CKD患者干预前后规范随访率和非计划再住院率的比较
Table 8. A comparative of the rates of standard follow-up and unplanned rehospitalization pre- and post-intervention among two groups of CKD patients
组别 例数 非计划再住院
[例(%)]规范随访率
[M(P25, P75),%]对照组 100 28(28.0) 71.15(50.00, 100.00) 干预组 97 15(15.5) 86.80(80.00,100.00) 统计量 4.535a 5.241b P值 0.033 <0.001 注:a为χ2值,b为Z值。
下载: 导出CSV
-
[1] CHEN T K, KNICELY D H, GRAMS M E. Chronic Kidney disease diagnosis and management: a review[J]. JAMA, 2019, 322(13): 1294-1304. doi: 10.1001/jama.2019.14745 [2] 李晓东, 周萍. 慢性肾脏病蛋白质能量消耗的发病机制及防治策略[J]. 实用临床医药杂志, 2021, 25(7): 118-122.LI X D, ZHOU P. Pathogenesis of protein energy wasting in chronic kidney disease and its prevention strategy[J]. Journal of Clinical Medicine in Practice, 2021, 25(7): 118-122. [3] STENGEL B, MUENZ D, TU C, et al. Adherence to the kidney disease: improving global outcomes CKD guideline in nephrology practice across countries[J]. Kidney Int Rep, 2020, 6(2): 437-448. [4] MA J W, WANG J Y, YING J P, et al. Long-term efficacy of an AI-based health coaching mobile app in slowing the progression of nondialysis-dependent Chronic Kidney disease: retrospective cohort study[J]. J Med Internet Res, 2024, 26: e54206. DOI: 10.2196/54206. [5] 应家佩, 戴丽丽, 马建伟, 等. 慢性肾脏病患者智能健康随访管理系统的构建及应用[J]. 护理学杂志, 2024, 39(19): 11-15, 30.YING J P, DAI L L, MA J W, et al. Construction and application of intelligent health follow-up management system for patients with chronic kidney disease[J]. Journal of Nursing Science, 2024, 39(19): 11-15, 30. [6] FISHER J D, FISHER W A, MISOVICH S J, et al. Changing AIDS risk behavior: effects of an intervention emphasizing AIDS risk reduction information, motivation, and behavioral skills in a college student population[J]. Health Psychol, 1996, 15(2): 114-123. doi: 10.1037/0278-6133.15.2.114 [7] KNOX J, KUTNER B A, SHIAU S, et al. Assessing the information-motivation-behavioral skills model to predict pre-exposure prophylaxis adherence among black men who have sex with men and transgender women in a community setting in New York City[J]. AIDS Behav, 2022, 26(7): 2494-2502. doi: 10.1007/s10461-022-03588-7 [8] JUNG W H, KIM H Y. Promoting foot self-care in type 2 diabetes mellitus patients receiving hemodialysis based on the information-motivation-behavioral skills model[J]. Nurs Health Sci, 2023, 25(4): 721-731. doi: 10.1111/nhs.13067 [9] LEE M H, PARK Y H. The effectiveness of the information-motivation-behavioral skills model-based intervention on preventive behaviors against respiratory infection among community-dwelling older adults[J]. Patient Educ Couns, 2021, 104(8): 2028-2036. doi: 10.1016/j.pec.2021.01.016 [10] NO A. KDIGO 2024 clinical practice guideline for the evaluation and management of Chronic Kidney disease[J]. Kidneys, 2024, 13(2): 140-171. doi: 10.22141/2307-1257.13.2.2024.456 [11] 于萍. 护理干预对慢性肾脏病患者自我管理及其健康状况影响的研究[D]. 天津: 天津医科大学, 2012.YU P. Study on the influence of nursing intervention on the self-management and health status of patients with chronic kidney disease[D]. Tianjin: Tianjin Medical University, 2012. [12] 上海市肾内科临床质量控制中心专家组. 慢性肾脏病早期筛查、诊断及防治指南(2022年版)[J]. 中华肾脏病杂志, 2022, 38(5): 453-464.Chinese Preventive Medisine Association For Kidney Disease. Guidelines for the early evaluation and management of chronic kidney disease in China(2022)[J]. Chinese Journal of Nephrology, 2022, 38(5): 453-464. [13] 韦昌韵, 郭雪洁, 赵培玉, 等. 肾移植受者自我管理现状及其相关影响因素研究[J]. 中华全科医学, 2022, 20(12): 2084-2087, 2137. doi: 10.16766/j.cnki.issn.1674-4152.002775WEI C Y, GUO X J, ZHAO P Y, et al. Analysis of related factors of self-management in kidney transplant recipients[J]. Chinese Joural of General Practice, 2022, 20(12): 2084-2087, 2137. doi: 10.16766/j.cnki.issn.1674-4152.002775 [14] 焦丽娟, 王婷, 李媛媛, 等. 血液透析联合血液灌流治疗慢性肾脏病终末期患者及对微炎症反应肾功能的影响[J]. 河北医学, 2023, 29(11): 1832-1837.JIAO L J, WANG T, LI Y Y, et al. Combination of hemodialysis and hemoperfusion for the treatment of end-stage chronic kidney disease patients and its impact on microinflammatory response and renal function[J]. Hebei Medicine, 2023, 29(11): 1832-1837. [15] WANG L M, XU X, ZHANG M, et al. Prevalence of chronic kidney disease in China: results from the sixth China chronic disease and risk factor surveillance[J]. JAMA Intern Med, 2023, 183(4): 298-310. doi: 10.1001/jamainternmed.2022.6817 [16] LEVIN A, AHMED S B, CARRERO J J, et al. Executive summary of the KDIGO 2024 Clinical Practice Guideline for the evaluation and management of chronic kidney disease: known knowns and known unknowns[J]. Kidney Int, 2024, 105(4): 684-701. doi: 10.1016/j.kint.2023.10.016 [17] LIU W, YU X J, WANG J Y, et al. Improving kidney outcomes in patients with nondiabetic chronic Kidney disease through an artificial intelligence-based health coaching mobile app: retrospective cohort study[J]. JMIR Mhealth Uhealth, 2023, 11: e45531. DOI: 10.2196/45531. [18] SCHECHTER M, JONGS N, CHERTOW G M, et al. Effects of dapagliflozin on hospitalizations in patients with chronic Kidney disease: a post hoc analysis of DAPA-CKD[J]. Ann Intern Med, 2023, 176(1): 59-66. doi: 10.7326/M22-2115 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 18
- HTML全文浏览量: 9
- PDF下载量: 3
- 被引次数: 0
