

Relationship blood routine and coagulation related indicators with short term prognosis of acute perforator atherosclerotic cerebral infarction
-
摘要:
目的 探讨血常规及凝血相关指标与急性穿支动脉粥样硬化性脑梗死近期预后的关系,以期为早期进行临床干预提供参考。 方法 选取2021年10月—2023年9月华北理工大学附属医院神经内科住院的303例急性穿支动脉粥样硬化性脑梗死患者作为研究对象,根据短期预后情况将患者分为预后良好组(189例)和预后不良组(114例)。比较2组患者血常规[平均血小板体积(MPV)、中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)]及凝血相关指标[凝血酶原时间(PT)、部分凝血活酶时间(APTT)、纤维蛋白原(FIB)],采用多因素logistic回归分析研究血常规及凝血相关指标与患者近期预后的关系,进一步通过ROC曲线分析其对预后的预测价值。 结果 预后不良组MPV、NLR、PLR、FIB较预后良好组明显增高(P<0.05),PT、APTT明显降低(P<0.05)。多因素回归分析显示,MPV、NLR、PLR、PT、APTT、FIB是患者预后不良的独立影响因素(P<0.05)。ROC曲线分析显示,MPV、NLR、PLR对患者预后不良均具有一定的预测效能,其中,NLR、PLR对诊断患者不良预后的曲线下面积分别为0.814(95% CI:0.763~0.865)、0.753(95% CI:0.695~0.811),两者相比,NLR对预后的预测价值较高(P=0.038);PT、APTT、FIB对患者近期预后不良均具有一定的预测效能,但三者的预测价值无明显差异。 结论 血常规及凝血相关指标与急性穿支动脉粥样硬化性脑梗死近期预后有关,临床可早期监测、干预,改善预后。 Abstract:Objective To explore the correlation of blood routine-related indexes and coagulation index-related markers with the short-term prognosis of acute perforator atherosclerotic cerebral infarction, in order to provide a reference for early clinical intervention. Methods A total of 303 patients admitted to our department of neurology from October 2021 to September 2023 were consecutively recruited, and according to their short-term prognosis, they were divided into a good prognosis group (189 cases) and a poor prognosis group (114 cases). The two groups were compared with blood routine-related indexes [mean platelet volume (MPV), neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR)] and coagulation index-related markers [prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen (FIB)]. Multivariate logistic regression analysis was applied to identify the relationship of the above indicators with the prognosis of acute perforator atherosclerotic cerebral infarction. ROC curve was plotted to analyze the predictive value of the indicators for disease prognosis in these patients. Results Compared with the good prognosis group, the MPV, NLR, PLR, and FIB in the poor prognosis group were significantly increased (P < 0.05), and the PT and APTT were significantly decreased (P < 0.05). Multivariate regression analysis showed that MPV, NLR, PLR, PT, APTT, and FIB were independent influencing factors for poor prognosis (P < 0.05). The results of ROC curve analysis showed that MPV, NLR, and PLR had certain predictive efficacy on the poor prognosis of patients. Among them, the area under the curve of NLR and PLR for predicting poor prognosis was 0.814 (95% CI: 0.763-0.865) and 0.753 (95% CI: 0.695-0.811), respectively. Compared with PLR, NLR had a significantly higher predictive value for prognosis (P=0.038). PT, APTT, and FIB all had certain predictive power for patients with poor prognosis in the near future, but there was no significant difference in the predictive value of the three. Conclusion MPV, NLR, PLR, PT, APTT, and FIB are associated with the short-term prognosis of acute perforator atherosclerotic cerebral infarction. Early monitoring and intervention can improve the prognosis. -
Key words:
- Acute cerebral infarction /
- Perforator atherosclerosis /
- Blood routine /
- Coagulation index /
- Prognosis
-

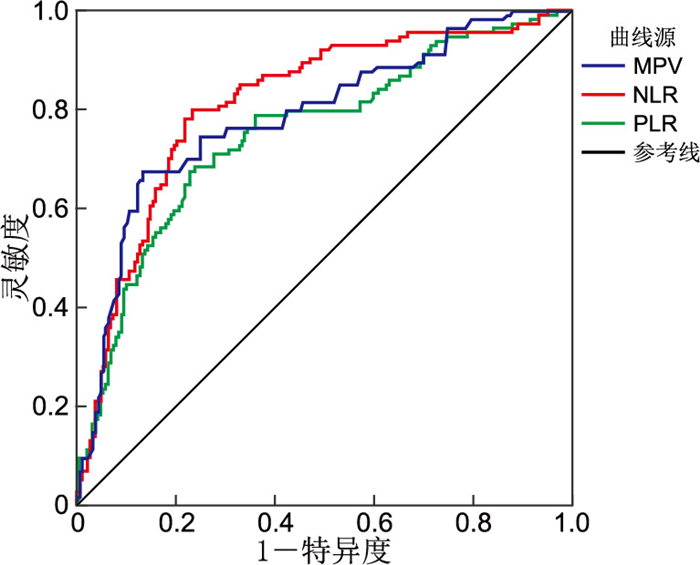
图 1 血常规指标预测脑梗死患者预后不良的ROC曲线
Figure 1. ROC curve analysis of blood routine indicators for predicting poor prognosis of patients with cerebral infarction

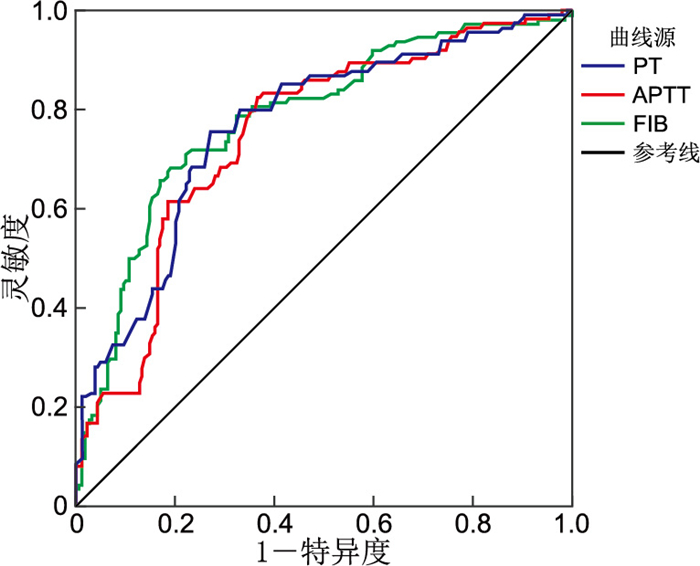
图 2 凝血功能指标预测患者预后不良的ROC曲线
Figure 2. ROC curve of coagulation function indicators for predicting poor prognosis of patients
表 1 预后良好组与预后不良组急性脑梗死患者一般情况比较
Table 1. Comparison of general conditions of patients with acute cerebral infarction between the good prognosis group and the poor prognosis group
组别 例数 性别[例(%)] 梗死部[例(%)] 吸烟[例(%)] 饮酒[例(%)] 高血压[例(%)] 糖尿病[例(%)] 冠心病[例(%)] 高脂血症[例(%)] 脑卒中史[例(%)] 男性 女性 前循环 后循环 预后不良组 114 71(62.3) 43(37.7) 71(62.3) 43(37.7) 54(47.4) 36(31.6) 86(75.4) 58(50.9) 16(14.0) 52(45.6) 52(45.6) 预后良好组 189 126(66.7) 63(33.3) 120(63.5) 69(36.5) 81(42.9) 58(30.7) 131(69.3) 52(27.5) 17(9.0) 73(38.6) 63(33.3) 统计量 0.601a 0.045a 0.586a 0.026a 1.313a 16.786a 1.861a 1.433a 4.554a P值 0.438 0.832 0.444 0.871 0.252 <0.001 0.172 0.231 0.033 组别 例数 年龄(x±s,岁) BMI(x±s) 入院时NIHSS评分(x±s,分) 入院时收缩压(x±s,mmHg) 入院时舒张压(x±s,mmHg) Hcy(x±s,μmol/L) TC(x±s,mmol/L) TG[M(P25,P75),mmol/L] LDL-C(x±s,mmol/L) HDL-C(x±s,mmol/L) 空腹血糖(x±s,mmol/L) UA(x±s,μmol/L) 预后不良组 114 64.62±4.02 25.90±3.50 5.53±2.50 152.65±19.24 94.79±11.86 18.72±6.87 5.33±1.21 1.63(1.20, 2.30) 3.81±0.88 1.27±0.23 8.28±4.11 318.24±85.29 预后良好组 189 64.01±3.25 25.40±3.32 3.62±1.53 151.89±18.35 93.04±12.92 17.07±8.25 4.99±1.14 1.43(1.10, 2.10) 3.32±0.85 1.21±0.27 6.96±3.26 306.77±81.15 统计量 1.388b 1.222b 7.372b 0.343b 1.175b 1.799b 2.470b -1.812c 4.823b 1.799b 2.915b 1.169b P值 0.167 0.223 <0.001 0.732 0.241 0.073 0.014 0.070 <0.001 0.073 0.004 0.243 组别 例数 TT(x±s,s) PLT(x±s,×109/L) PDW(x±s,%) D-二聚体(x±s,mg/L) MPV(x±s,fL) NLR(x±s) PLR(x±s) PT(x±s,s) APTT(x±s,s) FIB(x±s,g/L) 预后不良组 114 17.05±1.25 241.57±61.81 15.54±2.76 0.40±0.29 10.06±0.90 4.35±2.16 147.30±45.95 12.64±0.69 33.89±3.35 4.04±0.97 预后良好组 189 17.29±1.45 233.07±65.14 15.13±2.60 0.37±0.22 9.11±0.80 2.51±1.34 111.96±33.19 13.31±0.68 37.15±4.42 3.25±0.64 统计量 1.456b 1.122b 1.278b 1.164b 9.597b 8.192b 7.161b 8.278b 7.273b 7.648b P值 0.146 0.263 0.202 0.246 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 注:a为χ2值,b为t值,c为Z值。1 mmHg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 变量赋值情况
Table 2. Variable assignment
变量 赋值方法 糖尿病 无=0,有=1 脑卒中史 无=0,有=1 入院NIHSS评分 以实际值赋值 空腹血糖 以实际值赋值 TC 以实际值赋值 LDL-C 以实际值赋值 MPV 以实际值赋值 PT 以实际值赋值 APTT 以实际值赋值 FIB 以实际值赋值 NLR 以实际值赋值 PLR 以实际值赋值 是否预后不良 否=0,是=1
下载: 导出CSV
表 3 急性穿支动脉粥样硬化性脑梗死危险因素的多因素回归分析
Table 3. Multivariate regression analysis of risk factors for acute perforator atherosclerotic cerebral infarction
变量 B SE Waldχ2 P值 OR值 95% CI 糖尿病 0.870 0.437 3.962 0.047 2.386 1.013~5.617 脑卒中史 0.407 0.400 1.033 0.309 1.502 0.686~3.291 入院NIHSS评分 0.052 0.110 0.226 0.634 1.054 0.849~1.307 空腹血糖 0.088 0.053 2.802 0.094 1.092 0.985~1.210 TC 0.218 0.312 0.485 0.486 1.243 0.674~2.293 LDL-C 0.073 0.402 0.033 0.857 1.075 0.489~2.365 MPV 0.910 0.238 14.623 <0.001 2.483 1.558~3.958 PT -1.528 0.373 16.791 <0.001 0.217 0.104~0.451 APTT -0.118 0.058 4.096 0.043 0.889 0.793~0.996 FIB 0.642 0.264 5.883 0.015 1.899 1.131~3.190 NLR 0.294 0.143 4.210 0.040 1.342 1.013~1.776 PLR 0.024 0.006 17.021 <0.001 1.025 1.013~1.037
下载: 导出CSV
表 4 血常规指标预测脑梗死患者3个月预后的预测价值分析
Table 4. Predictive value analysis of routine blood indices for three-month prognosis in patients with cerebral infarction
项目 截断值 AUC 95% CI 灵敏度 特异度 P值 NLR 2.83 0.814 0.763~0.865 0.798 0.767 <0.001 PLR 122.45 0.753a 0.695~0.811 0.675 0.772 <0.001 MPV(fL) 9.84 0.788bc 0.734~0.843 0.675 0.868 <0.001 注:与NLR比较,aP=0.038,bP=0.472;与PLR比较,cP=0.401。
下载: 导出CSV
表 5 凝血功能指标对患者3个月预后的曲线分析
Table 5. Curve analysis of coagulation function indicators for three-month prognosis in patients
项目 截断值 AUC 95% CI 灵敏度 特异度 P值 PT(s) 12.91 0.768 0.712~0.823 0.754 0.730 <0.001 APTT(s) 35.85 0.751a 0.694~0.807 0.825 0.635 <0.001 FIB(g/L) 3.69 0.785bc 0.731~0.839 0.684 0.810 <0.001 注:与PT比较,aP=0.634,bP=0.638;与APTT比较,cP=0.336。
下载: 导出CSV
-
[1] MEN X J, HU M Y, GUO Z X, et al. Culprit plaques of large parent arteries, rather than cerebral small vessel disease, contribute to early neurological deterioration in stroke patients with intracranial branch atheromatous disease[J]. Cerebrovasc Dis, 2024, 53(1): 88-97. doi: 10.1159/000530371 [2] 陶涛, 何玲玲, 张业敏. 血常规中相关指标与急性脑梗死诊断及严重程度的相关性分析[J]. 中华全科医学, 2021, 19(10): 1717-1720, 1783. doi: 10.16766/j.cnki.issn.1674-4152.002150TAO T, HE L L, ZHANG Y M. Correlation analysis between relevant indexes and the diagnosis and severity of acute cerebral infarction in blood routine[J]. Chinese Journal of General Practice, 2021, 19(10): 1717-1720, 1783. doi: 10.16766/j.cnki.issn.1674-4152.002150 [3] 朱一珂, 杨君素, 钱芳, 等. 急性缺血性脑卒中患者血运重建前后NLR值与预后相关性分析[J]. 昆明医科大学学报, 2022, 43(8): 100-105.ZHU Y K, YANG J S, QIAN F, et al. Correlation analysis between NLR value and prognosis before and after revascularization in patients with acute ischemic stroke[J]. Journal of Kunming Medical University, 2022, 43(8): 100-105. [4] LIU Y L, WU K, XU R H, et al. Effect of mean platelet volume and platelet count on the prognosis of branch atheromatous disease[J]. Brain Behav, 2024, 14(5): e3509. DOI: 10.1002/brb3.3509. [5] ZHANG Y X, SHEN Z Y, JIA Y C, et al. The association of the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, lymphocyte-to-monocyte ratio and systemic inflammation response index with short-term functional outcome in patients with acute ischemic stroke[J]. J Inflamm Res, 2023, 16: 3619-3630. doi: 10.2147/JIR.S418106 [6] WOLBERG A S, SANG Y. Fibrinogen and factor XⅢ in venous thrombosis and thrombus stability[J]. Arterioscler Thromb Vasc Biol, 2022, 42(8): 931-941. doi: 10.1161/ATVBAHA.122.317164 [7] 门雪娇, 陈玮琪, 许玉园, 等. 穿支动脉粥样硬化病中国专家共识[J]. 中国卒中杂志, 2021, 16(5): 508-514.MEN X J, CHEN W Q, XU Y Y, et al. Chinese expert consensus on perforated atherosclerosis[J]. Chinese Journal of Stroke, 2021, 16(5): 508-514. [8] ZHENG Y Y, WANG L, SHI Q. Mean platelet volume (MPV)and platelet distribution width (PDW) predict clinical outcome of acute ischemic stroke: a systematic review and meta-analysis[J]. J Clin Neurosci, 2022, 101: 221-227. doi: 10.1016/j.jocn.2022.05.019 [9] LUDHIADCH A, YADAV P, SINGH S K, et al. Evaluation of mean platelet volume and platelet count in ischemic stroke and its subtypes: focus on degree of disability and thrombus formation[J]. Int J Neurosci, 2024, 134(5): 503-510. [10] GUAN J C, WANG Q, ZHAO Q S. Lymphocyte to monocyte ratio is independently associated with futile recanalization in acute ischemic stroke after endovascular therapy[J]. Neuropsychiatr Dis Treat, 2023, 19: 2585-2596. doi: 10.2147/NDT.S434225 [11] CHEN L C, ZHANG L L, LI Y D, et al. Association of the neutrophil-to-lymphocyte ratio with 90-day functional outcomes in patients with acute ischemic stroke[J]. Brain Sci, 2024, 14(3), 250. DOI: 10.3390/brainsci14030250. [12] KOLLIKOWSKI A M, PHAM M, MARZ A G, et al. Platelet activation and chemokine release are related to local neutrophil-dominant inflammation during hyperacute human stroke[J]. Transl Stroke Res, 2022, 13(3): 364-369. doi: 10.1007/s12975-021-00938-w [13] LIU C C, SHI D, NI X Q, et al. Correlations among lymphocyte count, white matter hyperintensity and brain atrophy in patients with ischemic stroke[J]. Front Aging Neurosci, 2025, 16: 1492078. DOI: 10.3389/fnagi,2024.1492078. [14] ZHU F, WANG Z H, SONG J H, et al. Correlation analysis of inflammatory markers with the short-term prognosis of acute ischaemic stroke[J]. Sci Rep, 2024, 14(1): 17772. DOI: 10.1038/s41598-024-66279-4. [15] YUAN Q F, YU L, WANG F. Efficacy of using thromboelastography to detect coagulation function and platelet function in patients with acute cerebral infarction[J]. Acta Neurol Belg, 2021, 121(6): 1661-1667. doi: 10.1007/s13760-020-01456-6 [16] CHEN Y, HAN L, ZHU D S, et al. Fibrinogen and neuroinflammation in the neurovascular unit in stroke[J]. J Inflamm Res, 2025, 18: 4567-4584. doi: 10.2147/JIR.S496433 [17] MEHTA V, SHARMA A, JYOTI D, et al. Fibrinogen as a predictor of early neurological deterioration in acute ischemic stroke-evidence from the Indian population[J]. J Cent Nerv Syst Dis, 2023, 37(10): 21-27. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 26
- HTML全文浏览量: 15
- PDF下载量: 5
- 被引次数: 0
