

Analysis of the development trajectory and influencing factors of symptom burden in perioperative patients with oral cancer
-
摘要:
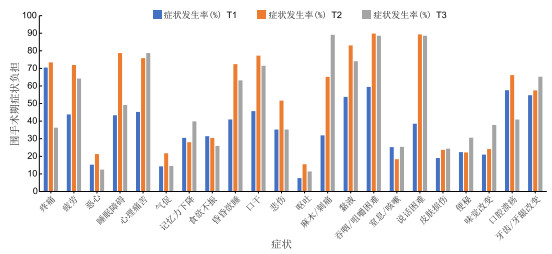
目的 调查不同阶段口腔癌围手术期患者的症状负担状况及动态变化,为临床工作人员制定症状管理策略提供依据。 方法 选取2021年1月—2023年12月于温州医科大学附属口腔医院及温州医科大学附属第一医院因诊断为口腔癌进行手术治疗的210例患者为研究对象。采用自制问卷、营养风险筛查2002及MD Anderson症状量表-头颈部模块-中文版量表分别在术前(T1)、术后7 d(T2)和出院后1个月(T3)对患者进行评估。采用广义估计方程分析口腔癌患者围手术期症状负担的变化轨迹及影响因素。 结果 T1时间节点有210份有效问卷、T2时间节点有207份有效问卷、T3时间节点有193份有效问卷。T1时间节点:显著存在的症状及发生率依次为疼痛(70.48%)、吞咽/咀嚼困难(59.52%)、口腔溃疡(57.62%)。T2时间节点:显著存在的症状及发生率依次为吞咽/咀嚼困难(89.85%)、说话困难(89.37%)、黏液问题(83.09%)。T3时间节点:显著存在的症状及发生率依次为麻木/刺痛(89.12%)、吞咽/咀嚼困难(88.60%)、说话困难(88.60%)。广义估计方程结果显示:合并症、晚期、NRS评分较高、接受辅助治疗的患者症状负担水平均较高(P<0.05)。 结论 口腔癌围手术期患者症状负担发生率较高,且症状负担随时间变化。应加强对合并症、肿瘤Ⅳ期、有营养风险的口腔癌患者症状负担的评估、监测和管理。 Abstract:Objective To investigate the status and evolutions of symptom burden among perioperative oral cancer patients at different stages of treatment, and to provide a scientific basis for developing targeted symptom management strategies. Methods A total of 210 patients diagnosed with oral cancer who underwent surgical treatment at the Affiliated Stomatology Hospital of Wenzhou Medical University and the First Affiliated Hospital of Wenzhou Medical University from January 2021 to December 2023 were selected as the study objects. Data were collected using self-designed questionnaires, the nutritional risk screening 2002, and the MD Anderson symptom scale-head and neck module (Chinese version). Assessments were conducted at three time points: before surgery (T1), 7 days after surgery (T2), and 1 month after discharge (T3). The trajectory and influencing factors of perioperative symptom burden in patients with oral cancer were analyzed by generalized estimation equation. Results A total of 210, 207, and 193 valid questionnaires were collected at T1, T2, and T3, respectively. At T1, the most common symptoms were pain (70.48%), difficulty in swallowing/chewing (59.52%), and mouth ulcers (57.62%). At T2, the predominant symptoms were difficulty in swallowing/chewing (89.85%), difficulty in speaking (89.37%), and mucus problems (83.09%). At T3, the main symptoms were numbness/tingling (89.12%), difficulty in swallowing/chewing (88.60%), and difficulty in speaking (88.60%). The results of generalized estimation equation showed that patients with occupational status as individuals, comorbidities, advanced stage, higher NRS score, and receiving adjuvant therapy experienced higher symptom burden (P < 0.05). Conclusion Perioperative oral cancer patients experience a high dynamic symptom burden that varies across disease stages. Clinical staff should strengthen the assessment, monitoring, and management of symptom burden, particularly for patients with comorbidities, stage Ⅳ disease, or oral nutritional risk, to improve overall postoperative outcomes. -
Key words:
- Oral cancer /
- Perioperative period /
- Symptom burden /
- Longitudinal study /
- Influencing factor
-

图 1 口腔癌患者T1~T3时间节点症状负担变化情况
Figure 1. Changes in symptom burden at T1-T3 time points in oral cancer patients
表 1 口腔癌患者3个时间点的症状发生率[例(%)]
Table 1. Symptom prevalence and severity at 3 time points in patients with oral cancer
症状 T1(n=210) T2(n=207) T3(n=193) 疼痛 148(70.48) 152(73.43) 70(36.27) 疲劳 92(43.81) 149(71.98) 124(64.25) 恶心 32(15.24) 44(21.25) 24(12.44) 睡眠障碍 91(43.33) 163(78.74) 95(49.22) 心理痛苦 95(45.24) 157(75.85) 152(78.76) 气促 30(14.29) 45(21.74) 28(14.51) 记忆力下降 64(30.48) 58(28.02) 77(39.90) 食欲不振 66(31.43) 63(30.43) 50(25.91) 昏昏欲睡 86(40.95) 150(72.46) 122(63.21) 口干 96(45.71) 160(77.29) 138(71.50) 悲伤 74(35.24) 107(51.69) 68(35.23) 呕吐 16(7.62) 32(15.46) 22(11.40) 麻木/刺痛 67(31.90) 135(65.22) 172(89.12) 黏液 113(53.81) 172(83.09) 143(74.09) 吞咽/咀嚼困难 125(59.52) 186(89.85) 171(88.60) 窒息/咳嗽 53(25.24) 38(18.36) 49(25.39) 说话困难 81(38.57) 185(89.37) 171(88.60) 皮肤损伤 40(19.05) 49(23.67) 47(24.35) 便秘 47(22.38) 46(22.22) 59(30.57) 味觉改变 44(20.95) 50(24.15) 73(37.82) 口腔溃疡 121(57.62) 137(66.18) 79(40.93) 牙齿/牙龈改变 115(54.76) 119(57.49) 126(65.28)  下载: 导出CSV
下载: 导出CSV
表 2 影响症状负担因素的广义估计方程参数估计结果
Table 2. Parameter estimates of generalized estimating equations for factors affecting symptom distress
项目 B SE Waldχ2 P值 95% CI 时间点 T2 17.741 2.572 47.886 <0.001 12.726~22.947 T3 2.633 1.856 2.044 0.152 -0.996~6.286 性别 女性 0.724 5.533 0.016 0.896 -10.134~112.602 年龄(岁) 45~59 0.567 4.136 0.018 0.892 -7.542~8.682 ≥60 -3.224 5.746 0.317 0.573 -14.459~8.052 文化程度 初中 1.628 3.105 0.274 0.599 -4.455~7.715 高中 4.749 3.633 1.708 0.192 -2.373~11.872 专科及以上 -1.221 7.183 0.028 0.864 -15.294~12.853 婚姻状况 有配偶 11.358 9.015 1.583 0.209 -6.322~28.894 居住地 乡镇 -1.593 4.685 0.116 0.733 -10.786~7.595 城市 -1.565 3.664 0.183 0.671 -8.750~5.622 职业 农民 5.286 3.537 2.235 0.136 -1.646~12.224 职员 -2.205 6.269 0.123 0.725 -14.493~10.082 已退休 -4.750 4.905 0.937 0.332 -14.360~4.862 个体 11.345 7.373 2.369 0.131 0.811~21.879 收入水平(元) 3 000~6 000 1.535 2.813 0.298 0.587 -3.984~7.052 >6 000 2.608 3.650 0.511 0.474 -4.546~9.760 保险类型 居民医保 -10.533 8.652 1.485 0.221 -27.384~6.552 职工医保 -7.295 9.468 0.592 0.440 -25.852~11.262 吸烟 是 -6.468 4.761 1.847 0.173 -15.795~2.863 饮酒 是 -1.778 4.270 1.175 0.672 -10.152~6.589 合并症 有 12.126 3.668 10.925 0.001 4.936~19.316 肿瘤分期 Ⅱ 6.715 3.216 4.360 0.036 0.412~13.023 Ⅲ 7.676 3.523 4.736 0.029 0.763~14.595 Ⅳ 13.870 3.337 17.265 <0.001 7.327~20.422 气管切开 是 1.442 3.202 0.204 0.650 -4.830~7.717 接受辅助治疗 是 6.789 3.258 4.341 0.037 0.401~13.177 体重指数 -0.665 0.514 1.662 0.197 -1.676~0.347 NRS营养风险筛查 3.680 1.040 12.530 <0.001 1.643~5.715 注:以时间点(T1)、性别(男性)、年龄(<45岁)、文化程度(小学及以下)、婚姻状况(无配偶)、居住地(农村)、职业(工人)、收入水平(<3 000元)、保险类型(无)、吸烟(否)、饮酒(否)、合并症(无)、肿瘤分期(Ⅰ期)、气管切开(否)、接受辅助治疗(否)为参照。
下载: 导出CSV
-
[1] BARRETT D, DUBAL R, L M C. The UK public and healthcare professionals' awareness of mouth cancer[J]. Br Dent J, 2023, 235(10): 811-815. doi: 10.1038/s41415-023-6490-5 [2] SUNG H, FERLAY J, SIEGEL R L, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249. [3] 冯娴, 姚元龙, 黄文博, 等. 全科医生对躯体症状障碍的识别与处理[J]. 中华全科医学, 2022, 20(3): 357-359. doi: 10.16766/j.cnki.issn.1674-4152.002352FENG X, YAO Y L, HUANG W B, et al. Recognition and management of somatic symptom disorder by general practitioners[J]. Chinese Journal of General Practice, 2022, 20(3): 357-359. doi: 10.16766/j.cnki.issn.1674-4152.002352 [4] 王瑾, 铁小伟, 付宝宝. 肺癌术后化疗患者血浆D-二聚体水平与癌因性疲乏及生活质量的关系研究[J]. 中国基层医药, 2024, 31(11): 1607-1611.WANG J, TIE X W, FU B B. Relationship between plasma D-dimer levels and cancer-caused fatigue and quality of life in postoperative chemotherapy patients with lung cancer[J]. Chinese Primary Medicine, 2024, 31(11): 1607-1611. [5] 朱小燕, 胡颖颖. 不同灸法对胃肠道肿瘤化疗患者癌因性疲乏的影响[J]. 中华全科医学, 2024, 22(6): 1051-1054.ZHU X Y, HU Y Y. Effects of different moxibustion methods on cancer-caused fatigue in patients undergoing chemotherapy for gastrointestinal tumors[J]. Chinese Journal of General Practice, 2024, 22(6): 1051-1054. [6] 高方方, 范平明, 吕鹏飞, 等. 乳腺癌患者选择腔镜或开放手术方式对术后生活质量的影响[J]. 新医学, 2024, 55(9): 708-715.GAO F F, FAN P M, LYU P F, et al. The impact of breast cancer patients' choice between endoscopic or open surgical methods on their postoperative quality of life[J]. Journal of New Medicine, 2024, 55(9): 708-715. [7] 刘红霞, 苏靖雯, 刘伟伟, 等. 围手术期胃癌患者症状群与生活质量的相关性研究[J]. 中国护理管理, 2023, 23(5): 680-685.LIU H X, SU J W, LIU W W, et al. Correlation between symptom clusters and quality of life in perioperative gastric cancer patients[J]. China Nursing Management, 2023, 23(5): 680-685. [8] 尚伟, 郑家伟. 2019年NCCN口腔口咽癌诊疗指南更新解读[J]. 中国口腔颌面外科杂志, 2019, 17(6): 481-485.SHANG W, ZHENG J W. Updated interpretation of the 2019 NCCN guidelines for the diagnosis and treatment of oral oropharyngeal cancer[J]. Chinese Journal of Oral and Maxillofacial Surgery, 2019, 17(6): 481-485. [9] HU Z Y, FENG X Q, FU M R, et al. Symptom patterns, physical function and quality of life among head and neck cancer patients prior to and after surgical treatment: a prospective study[J]. Eur J Oncol Nurs, 2020, 46: 101770. DOI: 10.1016/j.ejon.2020.101770. [10] 胡纯严, 胡良平. 合理进行均值比较: 重复测量设计定量资料方差分析[J]. 四川精神卫生, 2023, 36(z1): 7-12.HU C Y, HU L P. Rationalizing mean comparisons: an analysis of variance for quantitative data with repeated measures design[J]. Sichuan Mental Health, 2023, 36(z1): 7-12. [11] 程兰, 许庆珍, 李从玲, 等. 预后营养指数和NRS 2002评分对肺癌患者预后的临床研究[J]. 肿瘤代谢与营养电子杂志, 2021, 8(5): 534-538.CHENG L, XU Q Z, LI C L, et al. Prognostic nutritional index and NRS 2002 score on the prognosis of lung cancer patients[J]. Electronic Journal of Tumor Metabolism and Nutrition, 2021, 8(5): 534-538. [12] HANSEN C C, GUNN G B, MOHAMED A S R, et al. From patient-reported outcomes to quantitative health states: characterization of head and neck cancer patient survivorship utilities using prospective longitudinal assessment with the MDASI-HN[J]. Int J Radia Oncol, Biology, Physics, 2016, 94(4): 959-960. [13] HUTCHESON K A, WARNEKE C L, YAO C, et al. Dysphagia ater primary transoral robotic surgery with neck dissection vs nonsurgical therapy in patients with low- to intermediate-risk oropharyngeal cancer[J]. JAMA Otolaryngol Head Neck Surg, 2019, 145(11): 1053-1063. doi: 10.1001/jamaoto.2019.2725 [14] GRANT S, KAMAL M, MOHAMED A, et al. Single-item discrimination of quality-of-life-altering dysphagia among 714 long-term oropharyngeal cancer survivors: comparison of patient-reported outcome measures of swallowing[J]. Cancer, 2019, 125(10): 1654-1664. doi: 10.1002/cncr.31957 [15] SADAKANE-SAKURAMOTO A, HASEGAWA Y, SUGAHARA K, et al. Change in nutritional status and dysphagia after resection of head and neck cancer[J]. Nutrients, 2021, 13(7): 2438. DOI: 10.3390/nu13072438. [16] 张立杰, 关敏霞, 唐玲娟, 等. 术前气管推移训练联合术后徒手呼吸功能训练对颈椎前路手术患者术后吞咽功能和肺功能的影响[J]. 广西医学, 2021, 43(23): 2814-2817.ZHANG L J, GUAN M X, TANG L J, et al. Effects of preoperative tracheal pushover training combined with postoperative unarmed respiratory function training on postoperative swallowing function and lung function in patients undergoing anterior cervical spine surgery[J]. Guangxi Medicine, 2021, 43(23): 2814-2817. [17] GUILLEN-SOLA A, SOLER N B, MARCO E, et al. Effects of prophylactic swallowing exercises on dysphagia and quality of life in patients with head and neck cancer receiving (chemo) radiotherapy: the Redyor study, a protocol for a randomized clinical trial[J]. Trials, 2019, 20(1): 503. DOI: 10.1186/s13063-019-3587-x. [18] 陈青, 孙强, 冉芳. 下颌骨舌侧松解进路手术治疗口腔癌的临床疗效及对患者预后的影响[J]. 实用癌症杂志, 2023, 38(1): 101-104.CHEN Q, SUN Q, RAN F. Clinical efficacy of mandibular lingual release approach surgery for oral cancer and its effect on patients' prognosis[J]. Journal of Practical Cancer, 2023, 38(1): 101-104. [19] 叶海春, 高先连, 任阳, 等. 早期系统化康复训练在口腔癌术后游离皮瓣修复患者中应用效果的meta分析[J]. 中国口腔颌面外科杂志, 2020, 18(2): 171-176.YE H C, GAO X L, REN Y, et al. Meta-analysis of the effect of early systematic rehabilitation training in patients with postoperative free flap repair for oral cancer[J]. Chinese Journal of Oral and Maxillofacial Surgery, 2020, 18(2): 171-176. [20] BACHMANN A S, HÖCHE S, PETERS B, et al. Effects of high-frequency speech therapy on speech-related quality of life and objective speech intelligibility of oral cancer patients[J]. J Craniomaxillofac Surg, 2021, 49(11): 1072-1080. doi: 10.1016/j.jcms.2021.06.011 [21] ALLEN-AYODABO C O, ESKANDER A, DAVIS L E, et al. Symptom burden among head and neck cancer patients in the first year after diagnosis: association with primary treatment modality[J]. Oral Oncol, 2019, 99: 104434. DOI: 10.1016/j.oraloncology.2019.09.026. [22] MOTT F E, SACKS R, JOHNSON F, et al. Subjective functional outcomes in oropharyngeal cancer treated with induction chemotherapy using the MD Anderson Symptom Inventory (MDASI)[J]. Laryngoscope Investig Otolaryngol, 2020, 5(6): 1104-1109. doi: 10.1002/lio2.487 [23] 吴晓月, 韩宝瑾, 任似梦, 等. 头颈部肿瘤患者结束同步放化疗时症状负担和中医症状群分析[J]. 中医学报, 2023, 38(8): 1752-1757.WU X Y, HAN B J, REN S M, et al. Analysis of symptom burden and Chinese medicine symptom clusters in patients with head and neck tumors at the end of simultaneous radiotherapy[J]. Journal of Chinese Medicine, 2023, 38(8): 1752-1757. [24] 董瑜, 蒋莉莉. 口腔癌患者术后放疗期间营养相关症状的横断面调查[J]. 中国中西医结合耳鼻咽喉科杂志, 2023, 31(2): 151-154.DONG Y, JIANG L L. A cross-sectional survey of nutrition-related symptoms in oral cancer patients during postoperative radiotherapy[J]. Chinese Journal of Integrative Otolaryngology, 2023, 31(2): 151-154. -

 点击查看大图
点击查看大图
图(1) / 表(2)
计量
- 文章访问数: 10
- HTML全文浏览量: 2
- PDF下载量: 0
- 被引次数: 0
