

Correlation analysis between functional status and anxiety-depressive emotions in patients with ankylosing spondylitis
-
摘要:
目的 探讨强直性脊柱炎(AS)患者功能状态与焦虑抑郁情绪之间的关系,及AS临床用药在AS患者不同功能状态中对焦虑抑郁情绪的潜在影响。 方法 本研究纳入2021年3—6月就诊于解放军总医院第一医学中心风湿免疫科的148例AS患者。使用Bath强直性脊柱炎功能指数(BASFI)、Bath强直性脊柱炎测量指数(BASMI)评价患者的功能水平,抑郁自评量表(SDS)和焦虑自评量表(SAS)评价患者的情绪状态,探索AS患者功能水平与焦虑抑郁情绪的线性或非线性相关性,并按不同功能状态分组,分析AS常用药物的使用对AS患者合并焦虑抑郁情绪比例的潜在影响。 结果 AS患者中存在情绪问题者占比30.41%(45/148),其中合并焦虑、抑郁者占比分别为14.19%(21/148)和22.97%(34/148)。结果发现AS患者的BASFI与SAS和SDS评分呈显著线性相关(P < 0.001),而BASMI与SAS和SDS无相关性(P > 0.05)。亚组分析显示,BASFI<1.5的功能障碍亚组中,使用非甾体抗炎药(NSAIDs)治疗的AS患者合并抑郁情绪的比例更低(P=0.024),而肿瘤坏死因子拮抗剂、传统合成改善病情抗风湿药和中药的治疗对焦虑情绪影响的差异无统计学意义;药物对SAS的影响差异均无统计学意义。 结论 AS患者功能受限与焦虑抑郁情绪之间存在显著相关性。NSAIDs治疗可能改善有功能障碍AS患者的抑郁情绪状态。 Abstract:Objective To explore the relationship between functional status and anxiety-depressive emotions in patients with ankylosing spondylitis (AS), and to assess potential influences of clinical medications on anxiety-depressive emotions of AS patients in different functional status. Methods This study included 148 AS patients treated at Outpatient Rheumatology Clinics in the First Medical Center of Chinese PLA General Hospital from March 2021 to June 2021. The Bath ankylosing spondylitis functional index (BASFI) and Bath ankylosing spondylitis metrology index (BASMI) were used to evaluate the functional status, while the self-rating depression scale (SDS) and the self-rating anxiety scale (SAS) were utilized to assess the emotional disorder. Linear or nonlinear correlation between functional status and anxiety-depressive emotions was analyzed, and potential influences of different treatments on proportions of patients accompanied with anxiety-depressive emotions in subgroups based on functional status were investigated. Results Among included AS patients, 30.41% (45/148) were accompanied with emotional disorder, in which proportions of anxiety and depression were 14.19% (21/148) and 22.97% (34/148) respectively. Significant linear correlations were found between BASFI and scores of SAS and SDS (P < 0.001), while the correlation between BASMI and the scores of SAS and SDS was not statistically significant (P > 0.05). In functional limitation subgroup (BASFI < 1.5), AS patients treated with nonsteroidal anti-inflammatory drugs (NSAIDs) exhibited lower proportion of depression than those treated without NSAIDs (P=0.024), whereas impacts of tumor necrosis factor inhibitor, conventional synthetic disease modifying antirheumatic drug, and traditional Chinese medicine on SDS showed no significant difference. The effects of medications on anxiety were statistically non-different. Conclusion There are significant correlations between functional status and anxiety-depressive emotions in AS patients. Treatment with NSAIDs may improve the depressive emotional status of AS patients with functional limitation. -

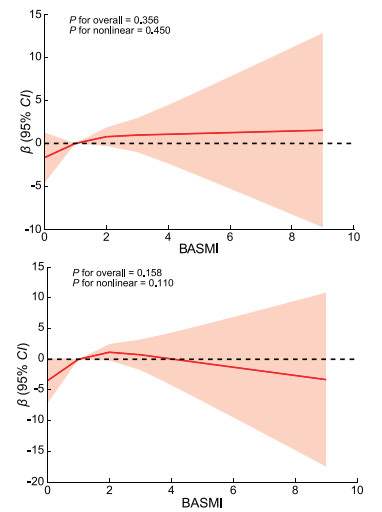
图 1 巴斯强直性脊柱炎测量指数与焦虑抑郁水平的限制性立方线条图
Figure 1. Restricted cubic spline of BASFI and scores of SAS and SDS
表 1 148例强直性脊柱炎患者一般资料
Table 1. Characteristics of 148 AS patients
项目 数值 年龄(x±s,岁) 33.79±8.51 性别(男性/女性,例) 121/27 吸烟[例(%)] 27(18.24) BMI(x±s) 24.33±3.67 AS评估 BASDAI(x±s) 1.85±1.44 ASDAS(x±s,分) 1.72±0.92 BASFI[M(P25, P75)] 1.00(0.20, 2.00) BASMI[M(P25, P75)] 1.00(0.00, 2.00) 红细胞沉降率[M(P25, P75),mm/h] 8.00(4.00, 18.00) C-反应蛋白[M(P25, P75),g/L] 3.04(1.00, 11.27) 情绪状态评估(x±s,分) SAS 39.99±9.48 SDS 42.27±11.96 药物使用[例(%)] NSASIDs 121(81.76) TNFi 50(33.78) csDMARDs 31(20.95) 中药 62(41.89) 注:NSAIDs为非甾体抗炎药(nonsteroidal anti-inflammatory drugs),TNFi为肿瘤坏死因子拮抗剂(tumor necrosis factor inhibitor),csDMARDs为传统合成改善病情抗风湿药(conventional synthetic disease modifying antirheumatic drug)。  下载: 导出CSV
下载: 导出CSV
表 2 NSAIDs对不同功能状态AS患者合并焦虑情绪的影响
Table 2. Effects of NSAIDs on anxiety in AS patients with different functional status
变量 NSAIDs(-) NSAIDs(+) β(95% CI) P值 全部患者 4/27 14/121 0.75(0.23~2.50) 0.642 功能正常组 1/18 5/76 0.14(-3.81~4.09) 0.695 功能障碍组 3/9 9/45 0.31(0.07~1.41) 0.130 注:全部患者与功能正常组比较,交互作用P=0.591。
下载: 导出CSV
表 3 TNFi对不同功能状态AS患者合并焦虑情绪的影响
Table 3. Effects of TNFi on anxiety in AS patients with different functional status
变量 TNFi(-) TNFi(+) β(95% CI) P值 全部患者 12/98 6/50 0.98(0.34~2.78) 0.966 功能正常组 4/61 1/33 0.45(0.05~4.16) 0.478 功能障碍组 8/37 5/17 1.51(0.41~5.57) 0.535 注:全部患者与功能正常组比较,交互作用P=0.355。
下载: 导出CSV
表 4 csDMARDs对不同功能状态AS患者合并焦虑情绪的影响
Table 4. Effects of csDMARDs on anxiety in AS patients with different functional status
变量 csDMARDs(-) csDMARDs(+) β(95% CI) P值 全部患者 16/117 2/31 0.44(0.09~2.00) 0.286 功能正常组 4/77 1/17 1.14(0.12~10.90) 0.909 功能障碍组 12/40 1/14 0.18(0.02~1.53) 0.116 注:全部患者与功能正常组比较,交互作用P=0.244。
下载: 导出CSV
表 5 中药对不同功能状态AS患者合并焦虑情绪的影响
Table 5. Effects of traditional Chinese medicine on anxiety in AS patients with different functional status
变量 中药(-) 中药(+) β(95% CI) P值 全部患者 8/86 10/62 1.88(0.69~5.06) 0.215 功能正常组 2/54 3/40 2.11(0.34~13.25) 0.426 功能障碍组 6/32 7/22 2.02(0.57~7.14) 0.274 注:全部患者与功能正常组比较,交互作用P=0.971。
下载: 导出CSV
表 6 NSAIDs对不同功能状态AS患者合并抑郁情绪的影响
Table 6. Effects of NSAIDs on depression in AS patients with different functional status
变量 NSAIDs(-) NSAIDs(+) β(95% CI) P值 全部患者 11/27 27/121 0.42(0.17~1.01) 0.052 功能正常组 3/18 9/76 0.67(0.16~2.78) 0.583 功能障碍组 8/9 18/45 0.08(0.01~0.72) 0.024 注:全部患者与功能正常组比较,交互作用P=0.114。
下载: 导出CSV
表 7 TNFi对不同功能状态AS患者合并抑郁情绪的影响
Table 7. Effects of TNFi on depression in AS patients with different functional status
变量 TNFi(-) TNFi(+) β(95% CI) P值 全部患者 24/98 14/50 1.20(0.56~2.59) 0.644 功能正常组 6/61 6/33 2.04(0.60~6.91) 0.254 功能障碍组 18/37 8/17 0.94(0.30~2.96) 0.914 注:全部患者与功能正常组比较,交互作用P=0.365。
下载: 导出CSV
表 8 csDMARDs对不同功能状态AS患者合并抑郁情绪的影响
Table 8. Effects of csDMARDs on depression in AS patients with different functional status
变量 csDMARDs(-) csDMARDs(+) β(95% CI) P值 全部患者 29/117 9/31 1.24(0.51~3.00) 0.631 功能正常组 9/77 3/17 1.62(0.39~6.75) 0.508 功能障碍组 20/40 6/14 0.75(0.22~2.56) 0.646 注:全部患者与功能正常组比较,交互作用P=0.423。
下载: 导出CSV
表 9 中药对不同功能状态AS患者合并抑郁情绪的影响
Table 9. Effects of traditional Chinese medicine on depression in AS patients with different functional status
变量 中药(-) 中药(+) β(95% CI) P值 全部患者 18/86 20/62 1.80(0.85~3.79) 0.122 功能正常组 6/54 6/40 1.41(0.42~4.75) 0.578 功能障碍组 12/32 14/22 2.92(0.95~8.99) 0.062 注:全部患者与功能正常组比较,交互作用P=0.390。
下载: 导出CSV
-
[1] TAUROG J D, CHHABRA A, COLBERT R A. Ankylosing spondylitis and axial spondyloarthritis[J]. N Engl J Med, 2016, 374(26): 2563-2574. doi: 10.1056/NEJMra1406182 [2] PARK J Y E, HOWREN A M, ZUSMAN E Z, et al. The incidence of depression and anxiety in patients with ankylosing spondylitis: a systematic review and meta-analysis[J]. BMC Rheumatol, 2020, 4: 12. DOI: 10.1186/s41927-019-0111-6. [3] ZHOU W, GUO J, HE M, et al. Fatigue and contributing factors in Chinese patients with ankylosing spondylitis[J]. Clin Rheumatol, 2020, 39(8): 2337-2344. doi: 10.1007/s10067-020-04976-x [4] 曹双燕, 邵战琴, 古洁若. 阿达木单抗治疗成年活动性强直性脊柱炎患者对其生存质量的影响[J]. 新医学, 2023, 54(6): 432-436.CAO S Y, SHAO Z Q, GU J R. Effect of adalimumab on quality of life in patients with active ankylosing spondylitis[J]. New Medicine, 2023, 54(6): 432-436. [5] ZOU Q, JIANG Y, MU F, et al. Correlation of axial spondyloarthritis with anxiety and depression[J]. Med Sci Monit, 2016, 22: 3202-3208. doi: 10.12659/MSM.897232 [6] OLE RINTEK M. Stability of fatigue, pain, patient global assessment and the Bath ankylosing spondylitis functional index (BASFI) in spondyloarthropathy patients with stable disease according to the Bath ankylosing spondylitis disease activity index (BASDAI)[J]. Rheumatol Int, 2018, 38(3): 425-432. doi: 10.1007/s00296-017-3920-1 [7] GEHAN E, AHMED A, SAHAR G, et al. Health-related quality of life in patients with ankylosing spondylitis: relationship with disease-related variables[J]. Curr Rheumatol Rev, 2019, 16(4): 311-318. [8] WANG L, SONG C, WANG Y, et al. Symptoms compatible with Rome Ⅳ functional bowel disorder in patients with ankylosing spondylitis[J]. Mod Rheumatol, 2023, 33(4): 823-829. doi: 10.1093/mr/roac064 [9] VAN WEELY S F, VAN DENDEREN J C, STEULTJENS M P, et al. Moving instead of asking? Performance-based tests and BASFI-questionnaire measure different aspects of physical function in ankylosing spondylitis[J]. Arthritis Res Ther, 2012, 14(2): R52. DOI: 10.1186/ar3765. [10] WARIAGHLI G, ALLALI F, BERRADA K, et al. Normative values for the bath ankylosing spondylitis functional index in the general population compared with ankylosing spondylitis patients in Morocco[J]. BMC Musculoskelet Disord, 2012, 13: 40. DOI: 10.1186/1471-2474-13-40. [11] SIEPER J, RUDWALEIT M, BARALIAKOS X, et al. The assessment of spondylo arthritis international society (ASAS) handbook: a guide to assess spondyloarthritis[J]. Ann Rheum Dis, 2009, 68 Suppl 2: ii1-44. DOI: 10.1136/ard.2008.104018. [12] DUNSTAN D A, SCOTT N. Norms for Zung's self-rating anxiety scale[J]. BMC Psychiatry, 2020, 20(1): 90. DOI: 10.1186/s12888-019-2427-6. [13] DONG HOON L, NANA K, FRANK B H, et al. Predicted lean body mass, fat mass, and all cause and cause specific mortality in men: prospective US cohort study[J]. BMJ, 2018, 362: k2575. DOI: 10.1136/bmj.k2575. [14] JIANG Y, YANG M, LV Q, et al. Prevalence of psychological disorders, sleep disturbance and stressful life events and their relationships with disease parameters in Chinese patients with ankylosing spondylitis[J]. Clin Rheumatol, 2018, 37(2): 407-414. doi: 10.1007/s10067-017-3907-z [15] AILEEN R N, GARETH T J, GARY J M, et al. Generating EQ-5D-5L health utility scores from BASDAI and BASFI: a mapping study in patients with axial spondyloarthritis using longitudinal UK registry data[J]. Eur J Health Econ, 2022, 23(8): 1357-1369. doi: 10.1007/s10198-022-01429-x [16] MARLIES C, DAVY P, LAURA van O, et al. Higher levels of physical activity are associated with less evasive coping, better physical function and quality of life in patients with axial spondyloarthritis[J]. PLoS One, 2024, 19(5): e0301965. DOI: 10.1371/journal.pone.0301965. [17] 李晏, 张胜利, 朱剑, 等. 盐酸度洛西汀治疗强直性脊柱炎伴抑郁患者的对照研究[J]. 中华医学杂志, 2013, 93(13): 966-969.LI Y, ZHANG S L, ZHU J, et al. Impact of duloxetine on depression and anxiety in patients with ankylosing spondylitis: a case-control study[J]. National Medical Journal of China, 2013, 93(13): 966-969. [18] VAN DER HEIJDE D, DEODHAR A, INMAN R D, et al. Comparison of three methods for calculating the Bath ankylosing spondylitis metrology index in a randomized placebo-controlled study[J]. Arthritis Care Res(Hoboken), 2012, 64(12): 1919-1922. doi: 10.1002/acr.21771 [19] YUE D, YIKAI D, MIN W, et al. Efficacy and acceptability of anti-inflammatory agents in major depressive disorder: a systematic review and meta-analysis[J]. Front Psychiatry, 2024, 15: 1407529. DOI: 10.3389/fpsyt.2024.1407529. [20] KHAI-JING N, KUANG-YUNG H, CHIEN-HSUEH T, et al. Risk factors, including different biologics, associated with depression and anxiety in patients with rheumatoid arthritis: a cross-sectional observational study[J]. Clin Rheumatol, 2019, 39(3): 737-746. [21] ECE U, ILKNUR K A, EZGI Ö, et al. The effects of methotrexate and biologics on the symptoms of depression and anxiety in patients with psoriasis[J]. Indian J Dermatol, 2023, 68(3): 237-244. doi: 10.4103/ijd.ijd_241_22 [22] 程鹏, 朱琦, 姜婷, 等. TNF-α拮抗剂对传统治疗反应欠佳的强直性脊柱炎患者生活质量的影响[J]. 中华全科医学, 2020, 18(3): 384-387, 431. doi: 10.16766/j.cnki.issn.1674-4152.001253CHENG P, ZHU Q, JIANG T, et al. Effect of TNF-α antagonist on quality of life of patients with ankylosing spondylitis who respond poorly to traditional treatments[J]. Chinese Journal of General Practice, 2020, 18(3): 384-387, 431. doi: 10.16766/j.cnki.issn.1674-4152.001253 [23] YUE T, LI Q, WANG R, et al. Comparison of hospital anxiety and depression scale (HADS) and Zung self-rating anxiety/depression scale (SAS/SDS) in evaluating anxiety and depression in patients with psoriatic arthritis[J]. Dermatology, 2020, 236(2): 170-178. doi: 10.1159/000498848 [24] GEORGE S A. Depression in the elderly[J]. Lancet, 2005, 365(9475): 1961-1970. doi: 10.1016/S0140-6736(05)66665-2 [25] DUAN S, REN Z, XIA H, et al. Associations between anxiety, depression with migraine, and migraine-related burdens[J]. Front Neurol, 2023, 14: 1090878. DOI: 10.3389/fneur.2023.1090878. [26] PARK J Y, HOWREN A M, ZUSMAN E Z, et al. The incidence of depression and anxiety in patients with ankylosing spondylitis: a systematic review and meta-analysis[J]. BMC Rheumatol, 2020, 4: 12. DOI: 10.1186/s41927-019-0111-6. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 10
- HTML全文浏览量: 3
- PDF下载量: 0
- 被引次数: 0
