

Analysis of risk factors of intrauterine distress in fetus
-
摘要:
目的 分析胎儿宫内窘迫的危险因素及这些因素对新生儿预后的影响,为临床干预提供依据。 方法 纳入2022年1月—2024年12月杭州市第一人民医院收治的107例胎儿宫内窘迫产妇(观察组)及107例同期正常妊娠产妇(对照组),比较2组新生儿的出生结局,并采用logistic回归分析和ROC曲线分析影响宫内窘迫发生的危险因素。 结果 单因素分析显示,脐血流异常、胎心率异常、胎动异常、羊水过少、脐带异常、胎盘早剥、妊娠期高血压、妊娠期糖尿病是影响胎儿发生宫内窘迫的危险因素(P<0.05);多因素logistic回归分析显示,胎心率异常、羊水过少、胎盘早剥、胎动异常及妊娠期糖尿病均是胎儿发生宫内窘迫的独立危险因素(P<0.05);ROC曲线分析发现,胎心率异常、羊水过少、胎盘早剥、胎动异常及妊娠期糖尿病预测发生宫内窘迫的AUC均大于0.7,且灵敏度(78.9%、72.6%、70.1%、63.2%、82.4%)和特异度(75.6%、69.3%、71.8%、74.5%、68.7%)较高。观察组中出现5 min Apgar评分<7分、新生儿窒息、低血糖、高胆红素血症及胎儿生长受限的例数均多于对照组,围产儿死亡率及NICU入住率亦高于对照组(P<0.05)。 结论 胎心率异常、羊水过少、胎盘早剥、胎动异常及妊娠期糖尿病是胎儿宫内窘迫的危险因素,上述因素易导致不良出生结局,需加强产前监测和围产期护理,以改善围产儿结局。 Abstract:Objective To analyze the risk factors of fetal intrauterine distress and their impact on neonatal prognosis, providing a basis for clinical intervention. Methods A total of 107 cases of intrauterine distress (observation group) and 107 normal pregnant women (control group) admitted to Hangzhou First People' s Hospital from January 2022 to December 2024 were enrolled, and the birth outcomes of neonates in the two groups were compared, and the risk factors affecting the occurrence of intrauterine distress were analyzed by logistic regression analysis and ROC working curve. Results Univariate analysis showed that abnormal umbilical cord blood flow, abnormal fetal heart rate, abnormal fetal movement, oligohydramnios, abnormal umbilical cord, placental abruption, gestational hypertension, and gestational diabetes mellitus were risk factors for fetal intrauterine distress (P < 0.05). Multivariate logistic regression analysis revealed that abnormal fetal heart rate, oligohydramnios, placental abruption, abnormal fetal movement, and gestational diabetes mellitus are independent risk factors for fetal distress (P < 0.05). ROC working curve analysis showed that the AUC of abnormal fetal heart rate, oligohydramnios, placental abruption, abnormal fetal movement and gestational diabetes mellitus was greater than 0.7, and the sensitivity (78.9%, 72.6%, 70.1%, 63.2%, 82.4%) and specificity (75.6%, 69.3%, 71.8%, 74.5%, 68.7%) were high. The 5-minute Apgar score was < 7 in the observation group, and the number of cases of neonatal asphyxia, hypoglycemia, hyperbilirubinemia, and fetal growth restriction were higher than those in the control group, and the perinatal mortality rate and Neonatal Intensive Care Unit (NICU) admission rate were also higher than those in the control group (P < 0.05). Conclusion Abnormal fetal heart rate, oligohydramnios, placental abruption, abnormal fetal movement, and gestational diabetes mellitus are risk factors for fetal intrauterine distress, and the above factors are likely to lead to adverse birth outcomes. Prenatal monitoring and perinatal care should be strengthened to improve perinatal outcomes. -
Key words:
- Fetal /
- Intrauterine distress /
- Risk factors /
- Prognosis
-

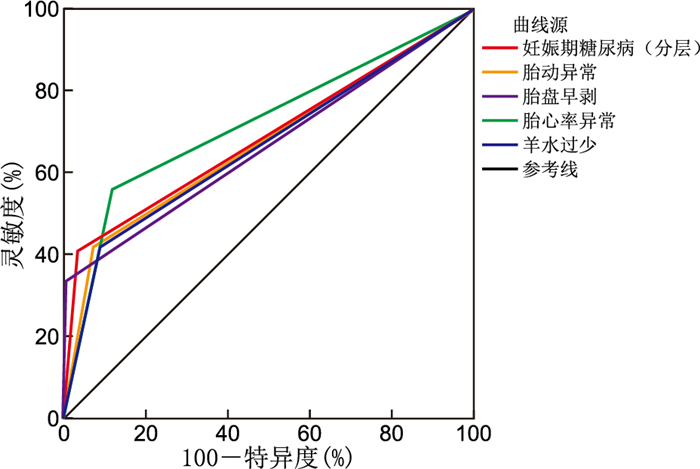
图 1 各因素预测胎儿宫内窘迫发生的ROC曲线
Figure 1. ROC curves for predicting fetal intrauterine distress based on various factors
表 1 2组研究对象基线资料与临床特征比较
Table 1. Comparison of baseline data and clinical characteristics between the two groups of study subjects
组别 例数 年龄(x±s,岁) 孕周
(x±s,周)BMI
(x±s)初产妇
[例(%)]妊娠期高血压
[例(%)]妊娠期糖尿病
[例(%)]观察组 107 30.5±4.2 37.8±2.1 26.5±3.4 73(68.2) 16(15.0) 18(16.8) 对照组 107 29.8±3.8 38.2±1.9 25.8±3.1 70(65.4) 9(8.4) 4(3.7) 统计量 1.192a 1.457a 1.354a 0.378b 4.067b 8.354b P值 0.234 0.145 0.178 0.542 0.043 0.004 组别 例数 羊水过少
[例(%)]脐带异常
[例(%)]胎盘早剥
[例(%)]脐血流异常
[例(%)]胎心率异常
[例(%)]胎动异常
[例(%)]观察组 107 24(22.4) 21(19.6) 10(9.3) 27(25.2) 32(29.9) 35(32.7) 对照组 107 10(9.3) 10(9.3) 1(0.9) 11(10.3) 13(12.1) 8(7.5) 统计量 7.982b 4.572b 7.762b 6.890b 8.571b 13.943b P值 0.005 0.032 0.005 0.009 0.003 <0.001 注:a为t值,b为χ2值。  下载: 导出CSV
下载: 导出CSV
表 2 胎儿发生宫内窘迫影响因素的单因素分析
Table 2. Univariate analysis of influencing factors of intrauterine distress in fetuses
变量 B SE Waldχ2 P值 OR值 95% CI 脐血流异常 1.032 0.402 6.632 0.010 2.807 1.284~6.138 胎心率异常 1.204 0.398 9.158 0.002 3.332 1.529~7.257 胎动异常 1.463 0.385 14.453 <0.001 4.318 2.031~9.182 羊水过少 1.138 0.362 9.867 0.002 3.120 1.533~6.349 脐带异常 0.832 0.385 4.685 0.030 2.298 1.079~4.909 胎盘早剥 1.506 0.521 8.353 0.004 4.510 1.625~12.532 妊娠期高血压 0.767 0.378 4.093 0.043 2.152 1.025~4.516 妊娠期糖尿病 1.325 0.432 9.321 0.002 3.762 1.613~8.772 注:各变量赋值如下,脐血流异常(有=1,无=0)、胎心率异常(有=1,无=0)、胎动异常(有=1,无=0)、羊水过少(有=1,无=0)、脐带异常(有=1,无=0)、胎盘早剥(有=1,无=0)、妊娠期高血压(有=1,无=0)、妊娠期糖尿病(有=1,无=0)。
下载: 导出CSV
表 3 胎儿发生宫内窘迫影响因素的多因素logistic回归分析
Table 3. Logistic regression analysis of factors influencing fetal intrauterine distress
变量 B SE Waldχ2 P值 OR值 95% CI 胎心率异常 1.125 0.415 7.341 0.006 3.077 1.363~6.939 羊水过少 1.043 0.375 7.789 0.005 2.837 1.353~5.944 胎盘早剥 1.523 0.545 7.798 0.005 4.583 1.570~13.398 胎动异常 0.986 0.402 6.085 0.014 2.679 1.217~5.902 妊娠期糖尿病 0.863 0.421 4.223 0.039 2.371 1.037~5.423
下载: 导出CSV
表 4 2组研究对象预后结局比较[例(%)]
Table 4. Comparison of prognostic outcomes between two groups of study subjects [cases (%)]
组别 例数 5 min Apgar评分<7分 NICU入住 新生儿窒息 新生儿低血糖 新生儿高胆红素血症 胎儿生长受限 围产儿死亡 观察组 107 20(18.7) 27(25.2) 14(13.1) 12(11.2) 15(14.0) 19(17.8) 6(5.6) 对照组 107 6(5.6) 10(9.3) 4(3.7) 3(2.8) 5(4.7) 8(7.5) 0 χ2值 8.354 8.571 6.890 5.274 5.135 4.762 6.171 P值 0.004 0.003 0.009 0.021 0.023 0.029 0.013
下载: 导出CSV
表 5 各因素对胎儿宫内窘迫的预测价值分析
Table 5. Analysis of the predictive value of various factors for intrauterine distress in the fetus
项目 AUC(95% CI) 灵敏度(%) 特异度(%) 约登指数 胎心率异常 0.780(0.715~0.845) 78.9 75.6 0.545 羊水过少 0.732(0.665~0.799) 72.6 69.3 0.419 胎盘早剥 0.728(0.661~0.795) 70.1 71.8 0.419 胎动异常 0.741(0.674~0.808) 63.2 74.5 0.377 妊娠期糖尿病(分层) 0.765(0.698~0.832) 82.4 68.7 0.511
下载: 导出CSV
-
[1] DAL MORO A P M, SOECKI G, DE FRAGA F S, et al. Fear of childbirth: prevalence and associated factors in pregnant women of a maternity hospital in southern Brazil[J]. BMC Pregnancy Childb, 2023, 23(1): 632. DOI: 10.1186/s12884-023-05948-0. [2] SINGH G, YADAV R, CHAKRAVARTY R. Understanding each other' s priorities: anesthesiologists versus gynecologists on fetal distress[J]. J Obstet Anaesth Cri, 2024, 14(2): 8. [3] 杨珏红, 张崇杰, 丁婷萍, 等. 血清SHBG与FABP4水平在妊娠期糖尿病患者早产风险中的交互影响及联合预测价值[J]. 河北医学, 2025, 31(5): 777-783.YANG Y H, ZHANG C J, DING T, et al. Interactive effect and combined predictive value of serum SHBG and FABP4 levels in the risk of preterm delivery in patients with gestational diabetes mellitus[J]. Hebei Medicine, 2025, 31(5): 777-783. [4] CHEN J, LIU F X, TAO R X. Relationship between ultrasound parameters of the umbilical and middle cerebral arteries and intrauterine fetal distress[J]. World J Clin Cases, 2024, 12(16): 2745-2750. doi: 10.12998/wjcc.v12.i16.2745 [5] 孔北华. 妇产科学[M]. 10版. 北京: 人民卫生出版社, 2024.KONG B H. Obstetrics and Gynecology[M]. 10th edition. Beijing: People' s Health Press, 2024. [6] 丁云, 王绪荣. 胎儿宫内窘迫的影响因素及其对新生儿出生结局的影响[J]. 临床医学, 2023(1): 42-44.DING Y, WANG X R. The influencing factors of fetal intrauterine distress and its impact on neonatal birth outcomes[J]. Clinical Medicine, 2023(1): 42-44. [7] ZHANG X G, PENG L Q, KUANG S Y, et al. Lactate accumulation from HIF-1α-mediated PMN-MDSC glycolysis restricts brain injury after acute hypoxia in neonates[J]. J Neuroinflamm, 2025, 22(1): 59. DOI: 10.1186/s12974-025-03385-8. [8] 刘铭忆, 马秀华. 妊娠期糖尿病妇女产后转归及随访的研究进展[J]. 中华全科医学, 2022, 20(1): 109-112, 116. doi: 10.16766/j.cnki.issn.1674-4152.002289LIU M Y, MA X H. Advance in research on postpartum outcome and follow-up of women with gestational diabetes mellitus[J]. Chinese Journal of General Practice, 2022, 20(1): 109-112, 116. doi: 10.16766/j.cnki.issn.1674-4152.002289 [9] SOFIA SOWJANYA M, SHAKUNTALA D S, LAKSHMI PRIYA Y, et al. Study of antepartum and intrapartum cardiotocography and fetal outcome in high risk pregnancy[J]. Cint J med Pub Health, 2024, 14(3). DOI: 10.70034/ijmedph.2024.3.24. [10] HAPDIJAYA I, SURYAWAN A, TESSALINA E, et al. Severe preeclampsia complicated by placental abruption leads to fetal distress[J]. J Kedokteran Meditek, 2023. DOI: 10.36452/jkdoktmeditek.v29i1.2432. [11] 中华医学会妇产科学分会产科学组. 早产临床防治指南(2024版)[J]. 中华妇产科杂志, 2024, 59(4): 257-269.Subgroup of Obstetrics, Society of Obstetrics and Gynecology, Chinese Medical Association. Clinical guidelines for the prevention and treatment of preterm birth (version 2024)[J]. Chinese Journal of Obstetrics and Gynecology, 2024, 59(4): 257-269. [12] CHAI L, LI S, YIN B B, et al. Prevalence, risk factors, and adverse perinatal outcomes in Chinese women with preeclampsia: a large retrospective cohort study[J]. J Health Popul Nutr, 2025, 44(1): 32. DOI: 10.1186/s41043-025-00778-6. [13] ZHANG J, MAO C, CAO Q, et al. Influencing factors of glycemic control in singleton pregnancies complicated by gestational diabetes mellitus in western China: a retrospective study[J]. Medicine, 2024, 103(38): 7. DOI: 10.1097/MD.0000000000039853. [14] KOPTEYEVA E V, SHELAYEVA E V, ALEKSEENKOVA E, et al. Fetal growth restriction in diabetic pregnancy: a retrospective single-center study Perinatal outcomes of pregnancies with borderline oligohydramnios at term[J]. J Obstet Womens Dis, 2023. DOI: 10.17816/jowd115018. [15] GUALTIERI S, SACCO M A, TARZIA P, et al. A rare case of maternal foetal death caused by uterine rupture in the placenta accreta[J]. Clin Ter, 2024, 175. DOI: 10.7417/CT.2024.5109. [16] SGAYER I, ELAFAWI M, BRAUDE O, et al. Fetal growth restriction in diabetic pregnancy: a retrospective single-center study Perinatal outcomes of pregnancies with borderline oligohydramnios at term[J]. Fetal Diagn Ther, 2025, 52(1). DOI: 10.1159/000541008. [17] NDIAYE M D, GUEYE M, MBODJI A, et al. Factors associated with oligohydramnios and related neonatal morbidity and mortality: a nested case-control study in a cohort[J]. Gynecol Obstet Res, 2024, 14(11): 1679-1686. [18] THIRUGNANASAMBANDAM R P, MUTHU J. Assessing maternal and perinatal complication incidence in pregnant patients with sickle cell disease: a retrospective analysis of transfusion therapy at a tertiary care hospital[J]. Blood, 2024, 144(Suppl 1): 5302. DOI: 10.1182/blood-2024-193389. [19] EVANS M I. Reconceptualizing intrauterine resuscitation and its short-term impact[J]. Diagnostics, 2025, 15. DOI: 10.3390/diagnostics15030255. [20] ZHU H B, WANG Y Y, YIN H W, et al. Risk factors associated with respiratory distress syndrome in late preterm infants[J]. Pak J Med Sci, 2024, 40(9): 1947-1952. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 12
- HTML全文浏览量: 5
- PDF下载量: 1
- 被引次数: 0
