

Intraoperative lithotripsy demand and its early predictive factors in patients undergoing laparoscopic common bile duct exploration
-
摘要:
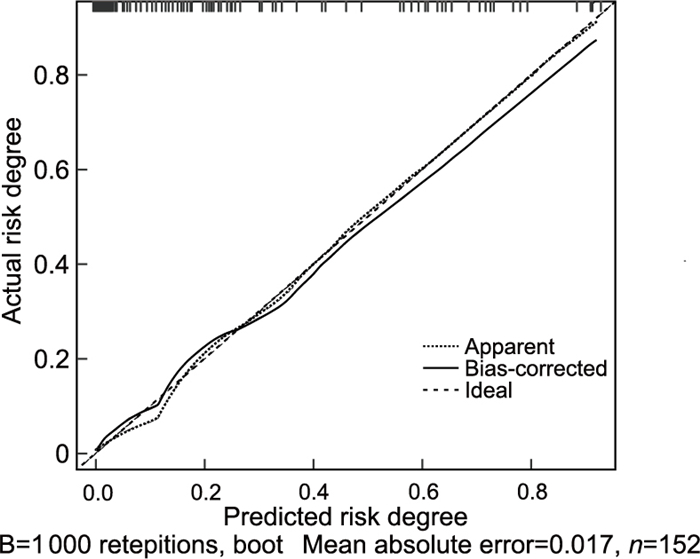
目的 探讨腹腔镜胆总管探查术(LCBDE)患者的术中碎石需求,并分析相关早期预测因素,以构建LCBDE术中碎石需求预测模型。 方法 纳入2022年3月—2024年3月浙江省人民医院淳安分院收治的152例LCBDE患者,根据术中腹腔镜下碎石辅助与否分为需求组(33例)和非需求组(119例)。比较2组患者一般资料、临床资料,采用多因素logistic回归分析研究LCBDE患者术中碎石需求的影响因素。 结果 需求组年龄、胆总管结石直径<1.1 cm占比均低于非需求组,发热、黄疸、恶心呕吐及胰腺周围渗出占比均高于非需求组(P<0.05)。多因素logistic回归分析显示,年龄(OR=0.824)、发热(OR=10.112)、黄疸(OR=8.071)、恶心呕吐(OR=5.823)、胆总管结石直径(OR=9.148)均为LCBDE患者术中碎石需求的独立影响因素(P<0.05)。基于五项指标构建的联合预测模型预测LCBDE患者术中碎石需求的AUC为0.914(95% CI:0.858~0.953),模型预测LCBDE患者术中碎石需求的发生风险与实际风险一致性良好。 结论 LCBDE用于胆总管结石治疗时,仍有部分患者术中需要碎石辅助;年龄、发热、黄疸、恶心呕吐和胆总管结石直径是术中碎石需求的独立影响因素,基于五项指标构建的联合预测模型可作为预测LCBDE患者术中碎石需求的临床工具。 Abstract:Objective To explore the lithotripsy demand of patients undergoing laparoscopic common bile duct exploration (LCBDE), and analyze the related early prediction factors, so as to build a prediction model of the lithotripsy demand during LCBDE. Methods One hundred and fifty-two patients with percutaneous LCBDE admitted to Chun' an Branch of Zhejiang Provincial People' s Hospital from March 2022 to March 2024 were divided into demand group (n=33) and non-demand group (n=119) according to the assistance of laparoscopic lithotripsy during operation. The general data and clinical data of patients in the two groups were compared, and the influencing factors of lithotripsy demand in patients with percutaneous LCBDE were analyzed by multivariate logistic regression. Results The ratio of age/common bile duct stone diameter < 1.1 cm in demand group was lower than that in non-demand group, and the ratio of fever, jaundice, nausea and vomiting and peripancreatic exudation was higher than that in non-demand group (P < 0.05). Multivariate logistic regression analysis showed that age (OR=0.824), fever (OR=10.112), jaundice (OR=8.071), nausea and vomiting (OR=5.823) and common bile duct stone diameter (OR=9.148) were the independent risk factors of lithotripsy demand in patients undergoing percutaneous LCBDE (P < 0.05). The ROC curve showed that the AUC of the combined model based on these five indicators was 0.914 (95% CI: 0.858-0.953), and the combined models predicted the risk of lithotripsy demand in patients with percutaneous LCBDE in good agreement with the actual risk. Conclusion There are still some patients who need lithotripsy during the treatment of choledocholithiasis by percutaneous LCBDE. Age, fever, jaundice, nausea and vomiting and the diameter of common bile duct stones are independent risk factors, and the combined prediction model based on these five indicators can be used as a clinical tool to predict the demand for lithotripsy in patients with percutaneous LCBDE. -
Key words:
- Laparoscopy /
- Common bile duct /
- Exploration /
- Gravel /
- Influencing factors /
- Calibration curve
-

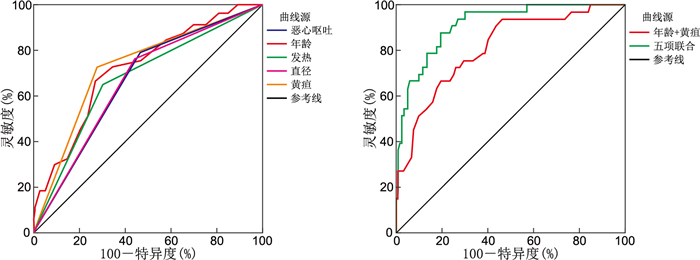
图 1 各指标预测经囊LCBDE患者术中碎石需求的ROC曲线
Figure 1. ROC curve of each indicator for predicting intraoperative lithotripsy demand of patients with percutaneous LCBDE

图 2 LCBDE患者术中碎石需求预测模型的校准曲线
Figure 2. Calibration curve of prediction model of lithotripsy demand in lcbde patients during operation
表 1 2组LCBDE患者临床资料比较
Table 1. Comparison of case data between the two groups of patients with LCBDE
项目 需求组(n=33) 非需求组(n=119) 统计量 P值 性别[例(%)] 0.240a 0.625 男性 16(48.48) 52(43.70) 女性 17(51.52) 67(56.30) 年龄(x±s, 岁) 47.36±5.02 52.07±6.14 4.531b <0.001 ASA分级[例(%)] 1.195a 0.274 Ⅰ级 21(63.64) 63(52.94) Ⅱ~Ⅲ级 12(36.36) 56(47.06) 腹部手术史[例(%)] 9(27.27) 25(21.01) 0.584a 0.445 ERCP[例(%)] 2(5.06) 4(3.36) 0.496a 0.481 临床表现[例(%)] 发热 20(60.61) 38(31.93) 10.934a <0.001 黄疸 21(63.64) 33(27.73) 14.541a <0.001 腹痛 20(60.61) 52(43.70) 2.963a 0.085 恶心呕吐 26(78.79) 55(46.22) 11.010a <0.001 基础疾病[例(%)] 肝脏疾病 1(3.03) 5(4.20) 0.093a 0.760 糖尿病 4(12.12) 12(10.08) 0.114a 0.736 高血压 10(30.30) 23(19.33) 1.831a 0.176 冠心病 2(6.06) 16(13.45) 1.667a 0.197 胆总管结石直径[例(%)] 10.624a 0.001 <1.1 cm 8(24.24) 67(56.30) ≥1.1 cm 25(75.76) 52(43.70) 胆囊周围渗出[例(%)] 3.053a 0.081 是 5(15.15) 7(5.88) 否 28(84.85) 112(91.12) 胰腺周围渗出[例(%)] 4.532a 0.033 是 8(24.24) 12(10.08) 否 25(75.76) 107(89.92) 胆总管直径(x±s, cm) 1.40±0.14 1.45±0.16 1.798b 0.084 淀粉酶[M(P25, P75), U/L] 47(39, 68) 62(45, 89) 1.942c 0.057 ALP[M(P25, P75), U/L] 178(131, 247) 157(88, 224) 1.779c 0.078 ALT[M(P25, P75), U/L] 146(89, 307) 102(41, 235) 1.123c 0.142 注:a为χ2值,b为t值,c为U值。  下载: 导出CSV
下载: 导出CSV
表 2 变量赋值情况
Table 2. Variable assignment
变量 赋值方法 术中是否辅助腹腔镜下碎石 是=1,否=0 年龄 以实际值赋值 发热 是=1,否=0 黄疸 是=1,否=0 恶心呕吐 是=1,否=0 胆总管结石直径 以实际值赋值 胰腺周围渗出 是=1,否=0
下载: 导出CSV
表 3 LCBDE患者术中碎石需求的多因素logistic回归分析
Table 3. Multivariate logistic regression analysis of intraoperative lithotripsy demand of LCBDE patients
变量 B SE Wald P值 OR值 95% CI 年龄 -0.194 0.060 10.404 0.001 0.824 0.732~0.927 发热 2.314 0.621 13.880 0.003 10.112 3.000~34.153 黄疸 2.088 0.576 13.151 <0.001 8.071 2.611~24.950 恶心呕吐 1.762 0.613 8.263 0.004 5.823 1.752~19.357 胆总管结石直径 2.214 0.657 11.337 0.001 9.148 2.522~33.183 胰腺周围渗出 1.003 0.705 2.028 0.154 2.727 0.685~10.851
下载: 导出CSV
表 4 各指标对LCBDE患者术中碎石需求的预测价值分析
Table 4. Analysis of the predictive value of each indicator for the intraoperative stone fragmentation requirements of LCBDE patients
项目 AUC 95% CI 灵敏度
(%)特异度
(%)Youden
指数年龄 0.723 0.644~0.792 66.67 73.11 0.398 发热 0.674 0.593~0.747 66.67 68.07 0.347 黄疸 0.725 0.647~0.794 72.73 72.27 0.450 恶心呕吐 0.663 0.582~0.737 78.79 53.78 0.326 胆总管结石直径 0.660 0.579~0.735 75.76 56.30 0.321 年龄+黄疸 0.812 0.741~0.871 93.94 53.78 0.477 联合预测模型 0.914 0.858~0.953 87.88 80.67 0.686
下载: 导出CSV
-
[1] ZDANOWICZ K, DANILUK J, LEBENSZTEJN D M, et al. The etiology of cholelithiasis in children and adolescents: a literature review[J]. Int J Mol Sci, 2022, 23(21): 13376. DOI: 10.3390/ijms232113376. [2] 李建军, 朱培欣, 陈锦州, 等. 以ALATS球囊行经皮经肝十二指肠乳头肌扩张顺行排石术治疗胆总管结石[J]. 中国介入影像与治疗学, 2023, 20(4): 202-206.LI J J, ZHU P X, CHEN J Z, et al. Treatment of choledocholithiasis with ALATS balloon percutaneous transhepatic papillary muscle dilation[J]. Chinese Journal of Interventional Imaging and Therapy, 2023, 20(4): 202-206. [3] 樊怡茹, 孙淑珍, 王红建. 经内镜乳头括约肌小切开联合球囊扩张术治疗老年胆总管结石患者的疗效与安全性分析[J]. 中国现代医学杂志, 2021, 31(6): 91-96.FAN Y R, SUN S Z, WANG H J. Efficacy and safety analysis of endoscopic sphincterotomy combined with balloon dilatation in the treatment of elderly patients with common bile duct stones[J]. China Journal of Modern Medicine, 2021, 31(6): 91-96. [4] CIANCI P, RESTINI E. Management of cholelithiasis with choledocholithiasis: endoscopic and surgical approaches[J]. World J Gastroenterol, 2021, 27(28): 4536-4554. doi: 10.3748/wjg.v27.i28.4536 [5] 王玉虎, 徐萌, 韩双喜, 等. 腹腔镜联合胆道镜经胆囊管汇入部微切开并一期缝合在胆总管探查取石术中的应用效果[J]. 临床医学研究与实践, 2021, 6(16): 61-63.WANG Y H, XU M, HAN S X, et al. The application effect of laparoscopy combined with choledochoscopy through the inlet of cystic duct and primary suture in common bile duct exploration and lithotomy[J]. Clinical Research and Practice, 2021, 6(16): 61-63. [6] SUWATTHANARAK T, AKARAVIPUTH T, PHALANUSITTHEPHA C, et al. Outcomes of laparoscopic common bile duct exploration by chopstick technique in choledocholithiasis[J]. JSLS, 2021, 25(2): e2021.00008. DOI: 10.4293/JSLS.2021.00008. [7] 马金玉, 吕超, 肖晶晶, 等. 胆总管微创手术取石后两种引流方式发生胆漏的危险因素及其预测模型建立[J]. 贵州医科大学学报, 2023, 48(1): 70-76.MA J Y, LYU C, XIAO J J, et al. Risk factors of bile leakage after minimally invasive choledocholithotomy by two drainage methods and its establishment of prediction model[J]. Journal of Guizhou Medical University, 2023, 48(1): 70-76. [8] DAS S, JHA A K, KUMAR M. Laparoscopic common bile duct exploration in cases of common bile duct stones: can LCBDE replace ERCP as first line treatment[J]. Am J Surg, 2023, 226(2): 290. DOI: 10.1016/j.amjsurg.2023.03.006. [9] 杨小勇, 张斌, 李文美, 等. 微爆破碎石在腹腔镜胆总管探查术治疗胆总管远端结石嵌顿中的应用效果[J]. 临床医学研究与实践, 2021, 6(1): 65-66, 72.YANG X Y, ZHANG B, LI W M, et al. Effect of micro-blasting lithotripsy in laparoscopic common bile duct exploration for incarcerated distal common bile duct stones[J]. Clinical Research and Practice, 2021, 6(1): 65-66, 72. [10] NARULA V K, FUNG E C, OVERBY D W, et al. Clinical spotlight review for the management of choledocholithiasis[J]. Surg Endosc, 2020, 34(4): 1482-1491. doi: 10.1007/s00464-020-07462-2 [11] 唐敏, 邵亚平, 杨蕾. 医护一体化模式在老年胆石症腹腔镜术后并发症预防中的应用[J]. 护理实践与研究, 2021, 18(12): 1856-1858.TANG M, SHAO Y P, YANG L. The application of integrated medical care model in the prevention of complications after laparoscopic cholecystectomy in the elderly[J]. Nursing Practice and Research, 2021, 18(12): 1856-1858. [12] 程尚美, 骆艳玲, 霍蕊. 快速康复外科护理技术在行ERCP的老年患者中的应用效果[J]. 中华全科医学, 2022, 20(3): 531-534. doi: 10.16766/j.cnki.issn.1674-4152.002394CHENG S M, LUO Y L, HUO R. Application effect of rapid rehabilitation surgical nursing technology in elderly patients undergoing ERCP[J]. Chinese Journal of General Practice, 2022, 20(3): 531-534. doi: 10.16766/j.cnki.issn.1674-4152.002394 [13] 周华波, 李广阔, 何伊嘉, 等. 三入路理论体系指导下的胆系结石病微创治疗研究进展[J]. 中国普通外科杂志, 2021, 30(2): 228-235.ZHOU H B, LI G K, HE Y J, et al. Research progress of minimally invasive treatment of cholelithiasis under the guidance of three-approach theory system[J]. Chinese Journal of General Surgery, 2021, 30(2): 228-235. [14] NAVARATNE L, MARTINEZ ISLA A. Transductal versus transcystic laparoscopic common bile duct exploration: an institutional review of over four hundred cases[J]. Surg Endosc, 2021, 35(1): 437-448. doi: 10.1007/s00464-020-07522-7 [15] NAVARATNE L, MARTíNEZ CECILIA D, MARTíNEZ ISLA A. The ABCdE score for predicting lithotripsy assistance during transcystic bile duct exploration by laparoendoscopy (PRE-LABEL)[J]. Surg Endosc, 2021, 35(11): 5971-5979. doi: 10.1007/s00464-020-08082-6 [16] MENG M, FENG H, TANG S, et al. Efficacy of ultrasound-guided percutaneous transhepatic biliary drainage for acute obstructive suppurative cholangitis combined with septic shock[J]. Clinics(Sao Paulo), 2023, 78(1): 100258. DOI: 10.1016/j.clinsp.2023.100258. [17] 王海方, 王旭阳, 兰涛. 腹腔镜联合胆道镜治疗胆囊及胆总管结石中转开腹列线图模型的建立[J]. 国际外科学杂志, 2021, 48(1): 9-15, F4.WANG H F, WANG X Y, LAN T. Establishment of laparotomy nomogram model in the treatment of gallbladder and common bile duct stones by laparoscopy combined with choledochoscope[J]. International Journal of Surgery, 2021, 48(1): 9-15, F4. [18] ZHENG Y, LV H, LIN Z, et al. A nomogram to predict conversion of laparoscopic surgery to laparotomy for choledocholithiasis[J]. BMC Surg, 2023, 23(1): 372. DOI: 10.1186/s12893-023-02275-1. [19] MA Z, ZHOU J, YAO L, et al. Safety and efficacy of laparoscopic common bile duct exploration for the patients with difficult biliary stones: 8 years of experiences at a single institution and literature review[J]. Surg Endosc, 2022, 36(1): 718-727. doi: 10.1007/s00464-021-08340-1 [20] 黄毅, 宁春玉, 黎结初, 等. 弥漫性大B细胞淋巴瘤预后预测模型的效能与外部验证[J]. 实用临床医药杂志, 2023, 27(17): 29-34, 39.HUANG Y, NING C Y, LI J C, et al. Efficacy and external validation of prognosis prediction model for diffuse large B-cell lymphoma[J]. Journal of Clinical Medicine in Practice, 2023, 27(17): 29-34, 39. [21] TUNRUTTANAKUL S, VERASMITH K, PATUMANOND J, et al. Development of a predictive model for common bile duct stones in patients with clinical suspicion of choledocholithiasis: a cohort study[J]. Gastroenterology Res, 2022, 15(5): 240-252. doi: 10.14740/gr1560 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 7
- HTML全文浏览量: 3
- PDF下载量: 0
- 被引次数: 0
