

Construction of risk model of esophageal and gastric varices rebleeding in cirrhosis based on 2D-SWE
-
摘要:
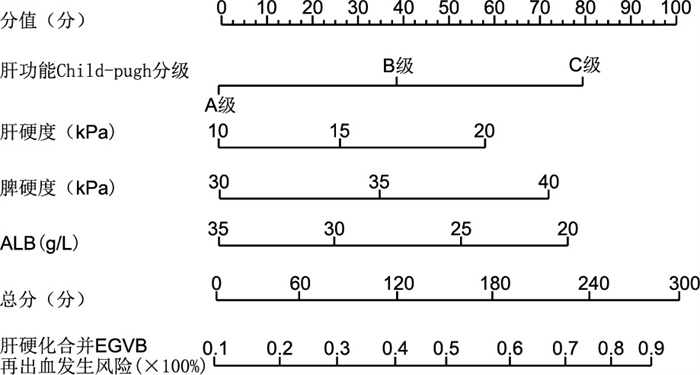
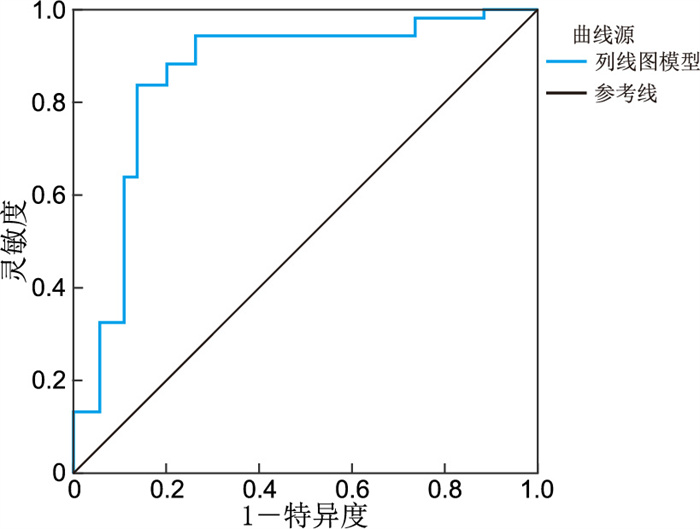
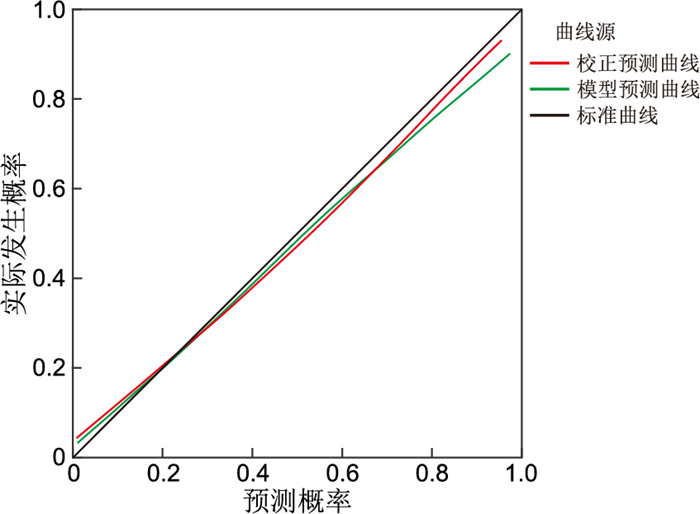
目的 肝硬化食管胃静脉曲张(EGV)再出血的病理生理机制复杂,且病死率高,明确其再出血的危险因素对降低病死率有重要作用。二维剪切波弹性成像(2D-SWE)能无创、定量地评估肝脏软硬程度,反映肝脏的病理改变。本研究基于2D-SWE构建EGV再出血风险模型,为临床防治提供参考。 方法 选取2020年1月—2022年12月郑州大学附属郑州中心医院收治的162例肝硬化EGV首次出血患者,根据患者是否发生再出血将其分为未再出血组(127例)和再出血组(35例)。采用logistic回归分析研究肝硬化患者EGV再出血的危险因素。构建肝硬化患者EGV再出血的列线图预测模型,并评估列线图模型预测效能。 结果 未再出血组肝功能Child-pugh分级A级、食管胃静脉曲张程度轻度、ALB水平较再出血组更高,未再出血组首次套扎、肝硬度、脾硬度较再出血组更低(P<0.05)。Logistic多因素回归分析结果显示,肝功能Child-pugh分级、肝硬度、脾硬度、ALB均是肝硬化发生EGV再出血的独立影响因素(P<0.05)。ROC曲线分析结果显示,列线图模型C-index指数为0.903(95% CI:0.846~0.975),列线图模型实测值与预测值基本一致,预测价值较高,具有较好的临床有效性。 结论 2D-SWE检测肝脾硬度是影响EGV再出血的危险因素,基于此构建的列线图预测模型对EGV再出血具有较好的预测效能。 Abstract:Objective The pathophysiological mechanism of esophageal and gastric varices (EGV) rebleeding in liver cirrhosis is complex, and the mortality rate is high. Identifying the literature factors of EGV rebleeding is important to reduce the mortality rate. Two-dimensional shear wave elastography (2D-SWE) can evaluate the degree of liver hardness and pathological changes in a non-invasive and quantitative manner. This study discusses the construction of the EGV rebleeding risk model based on 2D-SWE to provide a reference for clinical prevention and treatment. Methods A total of 162 patients with EGV with cirrhosis admitted to Zhengzhou Central Hospital Affiliated to Zhengzhou University from January 2020 to December 2022 were selected. According to whether rebleeding occurred, the patients were divided into the no rebleeding group (127 cases) and the rebleeding group (35 cases). The risk factors of EGV rebleeding in patients with cirrhosis were analyzed by Logistic regression. To construct a nomogram prediction model for the EGV rebleeding in cirrhotic patients, and evaluate the prediction efficiency of the nomogram model. Results The proportion of Child-pugh grade A liver function, the proportion of mild esophageal and gastric varices and the level of ALB in the group without rebleeding were higher than those in the group with rebleeding (P < 0.05), and the proportion of first ligation, liver hardness and spleen hardness in the group with no rebleeding were lower than those in the group with rebleeding (P < 0.05). Logistic multivariate results showed that Child-Pugh grade of liver function, liver hardness, spleen hardness, and ALB were independent influencing factors for EGV rebleeding in cirrhosis (P < 0.05). A nomogram model for predicting EGV rebleeding in cirrhosis was established according to the logistic multi-factor results, and the model was verified. ROC curve analysis results showed that the C-index of the nomogram model was 0.903 (95% CI: 0.846-0.975), and the measured value of the nomogram model was basically consistent with the predicted value, with high predictive value and good clinical effectiveness. Conclusion 2D-SWE detection of liver and spleen hardness is a risk factor for EGV rebleeding, and the prediction model based on this nomogram has a good predictive effect on EGV rebleeding. -
Key words:
- Liver cirrhosis /
- Esophagogastric varices /
- Rebleeding /
- Prediction model
-

图 3 肝硬化EGV再出血风险预测模型的ROC曲线
Figure 3. ROC curve of the risk prediction model for EGV rebleeding in cirrhosis

图 4 肝硬化发生EGV再出血风险预测模型的校准曲线
Figure 4. Calibration curve of the risk prediction model for EGV rebleeding in cirrhosis

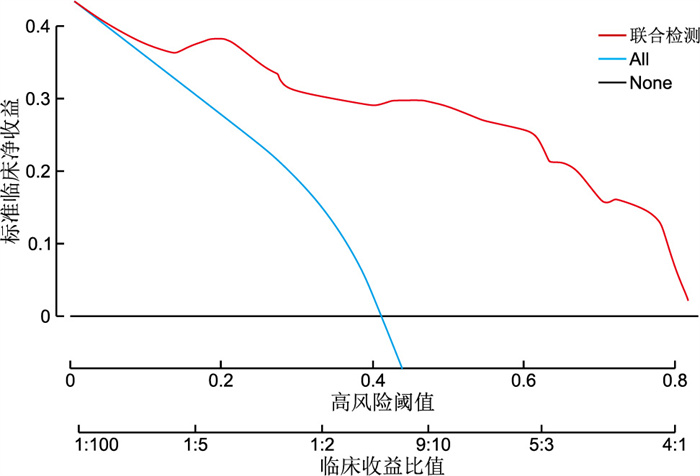
图 5 肝硬化发生EGV再出血风险预测模型决策曲线
Figure 5. Decision curve of risk prediction model for EGV rebleeding in cirrhosis
表 1 2组肝硬化食管胃底静脉曲张患者一般资料比较
Table 1. Comparison of general data of patients with esophageal and gastric varices in cirrhosis between the two groups
项目 未再出血组(n=127) 再出血组(n=35) 统计量 P值 性别[例(%)] 0.327a 0.567 男性 73(57.48) 22(62.86) 女性 54(42.52) 13(37.14) 年龄(x±s,岁) 52.36±7.69 54.55±8.93 1.439b 0.172 病因[例(%)] 0.450a 0.978 原发性胆汁性肝硬化 6(4.72) 2(5.71) 病毒性肝炎肝硬化 72(56.69) 18(51.43) 酒精性肝硬化 35(27.56) 10(28.57) 其他不明原因肝硬化 14(11.02) 5(14.29) 基础性疾病史[例(%)] 高血压病史 15(11.81) 4(11.43) 0.004a 0.950 糖尿病病史 8(6.30) 4(11.43) 1.053a 0.305 门静脉血栓 74(58.27) 16(45.71) 1.751a 0.186 其他 30(23.62) 11(31.43) 0.885a 0.347 肝功能Child-pugh分级[例(%)] -2.764c 0.017 A级 71(55.91) 10(28.57) B级 49(38.58) 22(62.86) C级 7(5.51) 3(8.57) 食管胃静脉曲张程度[例(%)] -2.566c 0.028 轻度 13(10.24) 0 中度 55(43.31) 11(31.43) 重度 59(46.46) 24(68.57) 是否腹水[例(%)] 0.710a 0.400 是 81(63.78) 25(71.43) 否 46(36.22) 10(28.57) 是否首次套扎[例(%)] 12.102a 0.001 是 33(25.98) 20(57.14) 否 94(74.02) 15(42.86) 门静脉内径(x±s,cm) 1.29±0.27 1.31±0.28 0.385b 0.701 肝硬度(x±s,kPa) 14.13±2.49 17.07±2.51 6.174b < 0.001 脾硬度(x±s,kPa) 32.05±3.23 36.09±3.25 5.814b < 0.001 WBC(x±s,×109/L) 5.18±1.33 4.78±1.25 1.595b 0.113 RBC(x±s,×1012/L) 4.05±1.02 3.68±0.93 1.935b 0.055 HB(x±s,g/L) 89.58±30.27 88.43±28.54 0.201b 0.841 PLT(x±s,×109/L) 145.21±60.45 135.49±55.32 0.857b 0.393 PA(x±s,mg/L) 95.32±35.33 82.79±35.16 7.045b 0.065 ALB(x±s,g/L) 32.15±8.91 24.03±8.79 4.787b < 0.001 Scr(x±s,μmol/L) 63.65±17.93 68.45±18.76 1.388b 0.167 PT(x±s,s) 14.28±3.79 15.16±4.82 1.144b 0.255 TBIL(x±s,μmol/L) 24.63±4.86 26.14±5.32 1.594b 0.113 AST(x±s,U/L) 46.15±14.39 51.28±16.32 1.813b 0.072 ALT(x±s,U/L) 31.42±10.32 35.33±12.42 1.896b 0.060 注:a为χ2值,b为t值,c为Z值。  下载: 导出CSV
下载: 导出CSV
表 2 肝硬化发生EGV再出血的logistic多因素回归分析
Table 2. Multi-factor analysis of EGV rebleeding in cirrhosis
变量 B SE Waldχ2 P值 OR值 95% CI 肝功能Child-pugh分级 0.735 0.284 6.698 <0.001 2.085 1.195~3.639 肝硬度 0.556 0.189 8.654 <0.001 1.744 1.025~2.462 脾硬度 0.579 0.167 12.021 <0.001 1.784 1.286~2.475 ALB -0.628 0.235 7.141 <0.001 0.534 0.337~0.846
下载: 导出CSV
-
[1] 张素媛, 李文雯, 朱娅琪, 等. 肝硬化相关肝性脑病患者血清中IL-6、IL-18与血氨水平的相关性分析[J]. 中华全科医学, 2023, 21(2): 288-291. doi: 10.16766/j.cnki.issn.1674-4152.002866ZHANG S Y, LI W W, ZHU Y Q, et al. Correlation analysis of serum IL-6, IL-18 and blood ammonia level in patients with hepatic encephalopathy[J]. Chinese Journal of General Practice, 2019, 21(2): 288-291. doi: 10.16766/j.cnki.issn.1674-4152.002866 [2] 陈秀, 余建平, 翁芳芳, 等. 授权教育饮食联合心理干预在病毒性肝炎后肝硬化中的应用[J]. 中华全科医学, 2022, 20(9): 1535-1537, 1586. doi: 10.16766/j.cnki.issn.1674-4152.002642CHEN X, YU J P, WENG F F, et al. Authorised educational diet combined with psychological intervention in viral post-hepatitis cirrhosis[J]. Chinese Journal of General Practice, 2022, 20(9): 1535-1537, 1586. doi: 10.16766/j.cnki.issn.1674-4152.002642 [3] KAPLAN D E, RIPOLL C, THIELE M, et al. AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis[J]. Hepatology, 2024, 79(5): 1180-1211. doi: 10.1097/HEP.0000000000000647 [4] JOTHIMANI D, RELA M, KAMATH P S. Liver cirrhosis and portal hypertension: how to deal with esophageal varices?[J]. Med Clin North Am, 2023, 107(3): 491-504. doi: 10.1016/j.mcna.2023.01.002 [5] GUO H W, XIAO J Q, WANG Y, et al. Increase in free hepatic venous pressure response to beta-blockers predicts variceal bleeding in cirrhotic patients[J]. Biomed Res Int, 2021, 2021: 5587566. DOI: 10.1155/2021/5587566. [6] 汪克文, 郑健荪, 张忠杰, 等. 多层螺旋CT指标对普萘洛尔治疗的肝硬化患者发生食管静脉曲张出血的预测意义[J]. 贵州医科大学学报, 2025, 50(3): 461-468.WANG K W, ZHENG J S, ZHANG Z J, et al. Predictive value of multislice spiral CT indicators for propranolol prophylactic treatment of esophageal variceal bleeding of patients with liver cirrhosis[J]. Journal of Guizhou Medical University, 2025, 50(3): 461-468. [7] KARAGIANNAKIS D S, MARKAKIS G, LAKIOTAKI D, et al. Comparing 2D-shear wave to transient elastography for the evaluation of liver fibrosis in nonalcoholic fatty liver disease[J]. Eur J Gastroenterol Hepatol, 2022, 34(9): 961-966. doi: 10.1097/MEG.0000000000002412 [8] WANG P, HU X H, XIE F. Predictive value of liver and spleen stiffness measurement based on two-dimensional shear wave elastography for the portal vein pressure in patients with compensatory viral cirrhosis[J]. Peer J, 2023, 11: e15956. DOI: 10.7717/peerj.15956. [9] HU C, LIANG S, LIU H H, et al. Prediction of ablation zone disappearance after microwave ablation for the patients with papillary thyroid microcarcinoma using nomograph[J]. Front Endocrinol, 2023, 14: 1145958. DOI: 10.3389/fendo.2023.1145958. [10] WANG Y T, SHAO Q, LUO S Y, et al. Development of a nomograph integrating radiomics and deep features based on MRI to predict the prognosis of high grade Gliomas[J]. Math Biosci Eng, 2021, 18(6): 8084-8095. doi: 10.3934/mbe.2021401 [11] 中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会内镜学分会. 肝硬化门静脉高压食管胃静脉曲张出血的防治指南[J]. 中国肝脏病杂志(电子版), 2016, 8(1): 1-18.Chinese Society of Hepatology, Chinese Society of Gastroenterology, Chinese Society of Endoscopy. Guideline for the diagnosis and treatment of esophageal and gastric variceal bleeding in cirrhotic portal hypertension[J]. Chinese Journal of Liver Diseases(Electronic Version), 2016, 8(1): 1-18. [12] ALBILLOS A, MARTIN-MATEOS R, VAN DER MERWE S, et al. Cirrhosis-associated immune dysfunction[J]. Nat Rev Gastroenterol Hepatol, 2022, 19(2): 112-134. doi: 10.1038/s41575-021-00520-7 [13] ENGELMANN C, CLÀRIA J, SZABO G, et al. Pathophysiology of decompensated cirrhosis: portal hypertension, circulatory dysfunction, inflammation, metabolism and mitochondrial dysfunction[J]. J Hepatol, 2021, 75(Suppl 1): S49-S66. [14] HOU Y X, YU H, ZHANG Q, et al. Machine learning-based model for predicting the esophagogastric variceal bleeding risk in liver cirrhosis patients[J]. Diagn Pathol, 2023, 18(1): 29. DOI: 10.1186/s13000-023-01293-0. [15] WU K N, FU Y F, GUO Z X, et al. Analysis of the timing of endoscopic treatment for esophagogastric variceal bleeding in cirrhosis[J]. Front Med, 2022, 9: 1036491. DOI: 10.3389/fmed.2022.1036491. [16] LIU H M, ZHANG Q, GAO F Y, et al. Platelet count/spleen thickness ratio and the risk of variceal bleeding in cirrhosis with esophagogastric varices[J]. Front Med, 2022, 9: 870351. DOI: 10.3389/fmed.2022.870351. [17] DUAN X W, HE X, YAN H Z, et al. Analysis of complications and risk factors other than bleeding before and after endoscopic treatment of esophagogastric variceal bleeding in patients with liver cirrhosis[J]. Can J Gastroenterol Hepatol, 2023, 2023: 7556408. DOI: 10.1155/2023/7556408. [18] ZHANG W H, WANG Y L, CHU J D, et al. Investigation report on endoscopic management of esophagogastric variceal bleeding by Chinese endoscopists[J]. Medicine, 2022, 101(42): e31263. DOI: 10.1097/MD.0000000000031263. [19] CAO R, LU X Y, WU Y L, et al. Laparoscopic splenectomy and esophagogastric devascularization versus endoscopic varices ligation plus laparoscopic splenectomy in the treatment of portal hypertension[J]. J Laparoendosc Adv Surg Tech A, 2023, 33(11): 1052-1057. doi: 10.1089/lap.2023.0243 [20] LIN L Y, ZENG D W, LIU Y R, et al. Diagnostic value of liver stiffness measurement combined with risk scores for esophagogastric variceal bleeding in patients with hepatitis B cirrhosis[J]. Eur J Radiol, 2024, 173: 111385. DOI: 10.1016/j.ejrad.2024.111385. [21] WANG P, WU P, JIA B B, et al. Analysis of the predictive value of real-time shear wave elastography in detecting the elastic hardness of liver and spleen in patients with portal hypertension of hepatitis B cirrhosis[J]. Panminerva Med, 2023, 65(4): 538-539. [22] HU X G, DAI J J, LU J, et al. Efficacy of transjugular intrahepatic portosystemic shunts in treating cirrhotic esophageal-gastric variceal bleeding[J]. World J Gastrointest Surg, 2024, 16(2): 471-480. doi: 10.4240/wjgs.v16.i2.471 [23] 邝小红, 吴曼丽. 声触诊弹性成像与肝脏纤维化评分评估肝硬化高风险食管静脉曲张的比较[J]. 新医学, 2025, 56(11): 1116-1122.KUANG X H, WU M L. Comparison of sound touch elastography and liver fibrosis scores in assessing high-risk esophageal varices in patients with liver cirrhosis[J]. Journal of New Medicine, 2025, 56(11): 1116-1122. [24] LV J, LIU Y Y, JIA Y T, et al. A nomogram model for predicting prognosis of obstructive colorectal cancer[J]. World J Surg Oncol, 2021, 19(1): 337. DOI: 10.1186/s12957-021-02445-6. [25] 胡明洁, 张凤英, 刘慧影. 超敏cTnT与血栓-炎症因子的相关性及其对急性缺血性脑卒中神经功能结局的预测价值[J]. 新医学, 2021, 52(3): 203-207.HU M J, ZHANG F Y, LIU H Y. Relationship between high-sensitivity cardiac troponin T and thrombo-inflammatory molecules and its value in predicting neurological function outcome after acute ischemic stroke[J]. Journal of New Medicine, 2021, 52(3): 203-207. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 11
- HTML全文浏览量: 4
- PDF下载量: 0
- 被引次数: 0
