

Predictive value of serum TSPO, BDNF, and TNF-α levels for post-stroke depression in patients with acute ischemic stroke
-
摘要:
目的 评估血清18 kDa易位蛋白(TSPO)、脑源性神经营养因子(BDNF)、肿瘤坏死因子-α(TNF-α)水平对急性缺血性卒中(AIS)患者发生卒中后抑郁(PSD)的临床意义。 方法 选取2022年1月—2024年1月新乡医学院第一附属医院收治的121例AIS患者,根据出院后3个月17项汉密尔顿抑郁量表(HDRS-17)评估是否出现PSD,将其分为PSD组(38例)和非PSD组(83例)。收集2组患者的人口学资料、临床特征,并比较2组患者血清TSPO、BDNF、TNF-α水平差异。采用logistic回归分析筛选PSD的独立危险因素,并绘制ROC曲线评估血清TSPO、BDNF、TNF-α水平联合检测对PSD的预测价值。 结果 PSD组患者血清TSPO、TNF-α水平高于非PSD组(P<0.05),而BDNF水平低于非PSD组(P<0.05)。Logistic回归分析显示,血清TSPO水平升高(OR=2.065,95% CI:1.052~4.055,P<0.05)、TNF-α水平升高(OR=1.374,95% CI:1.031~1.832,P<0.05)均是PSD的危险因素,而BDNF水平升高(OR=0.696,95% CI:0.521~0.929,P<0.05)是PSD的保护因素。ROC曲线分析显示,血清TSPO、BDNF、TNF-α水平联合检测对PSD的预测效能良好,AUC为0.797。 结论 血清TSPO、BDNF、TNF-α水平与AIS患者发生PSD密切相关,联合检测这3种生物标志物可能有助于早期识别PSD高危人群,为临床预防和治疗PSD提供依据。 -
关键词:
- 急性缺血性卒中 /
- 卒中后抑郁 /
- 18 kDa易位蛋白 /
- 脑源性神经营养因子 /
- 肿瘤坏死因子-α
Abstract:Objective To investigate the predictive value of serum translocator protein 18 kDa (TSPO), brain-derived neurotrophic factor (BDNF), and tumor necrosis factor-α (TNF-α) levels for post-stroke depression (PSD) in patients with acute ischemic stroke (AIS). Methods A total of 121 AIS patients admitted to the First Affiliated Hospital of Xinxiang Medical University from January 2022 to January 2024 were enrolled in this study. Based on the 17-item Hamilton depression rating scale assessment at 3 months after discharge, patients were divided into PSD group (n=38) and non-PSD group (n=83). Demographic data, clinical characteristics, and serum levels of TSPO, BDNF, and TNF-α were compared between the two groups. Logistic regression analysis was used to identify independent risk factors for PSD, and a receiver operating characteristic (ROC) curve was constructed to evaluate the predictive value of combined detection of serum TSPO, BDNF, and TNF-α levels for PSD. Results Serum TSPO and TNF-α levels were significantly higher in the PSD group than those in the non-PSD group (P < 0.05), while BDNF levels were significantly lower in the PSD group (P < 0.05). Logistic regression analysis showed that elevated serum TSPO (OR=2.065, 95% CI: 1.052-4.055, P < 0.05) and TNF-α (OR=1.374, 95% CI: 1.031-1.832, P < 0.05) levels were risk factors for PSD, while elevated BDNF level (OR=0.696, 95% CI: 0.521-0.929, P < 0.05) was a protective factor. ROC curve analysis showed that the combined detection of serum TSPO, BDNF, and TNF-α levels had a good predictive value for PSD, with an area under the curve of 0.797. Conclusion Serum TSPO, BDNF, and TNF-α levels are closely related to the development of PSD in patients with AIS. The combined detection of these three biomarkers may be helpful for early identification of high-risk populations for PSD, providing a basis for clinical prevention and treatment of PSD. -

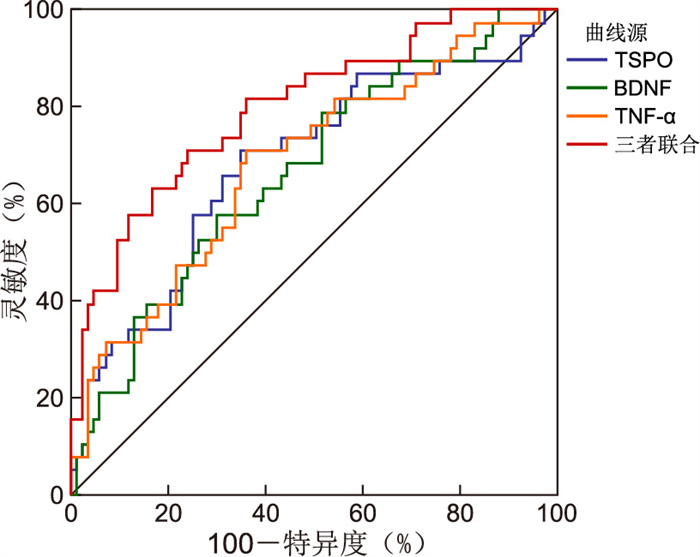
图 1 血清TSPO、BDNF和TNF-α预测AIS患者发生PSD的ROC曲线
Figure 1. ROC curve of serum TSPO, BDNF and TNF-α in predicting PSD of AIS patients
表 1 2组AIS患者基线资料比较
Table 1. Comparison of baseline data between the two groups of AIS patients
项目 PSD组(n=38) 非PSD组(n=83) 统计量 P值 年龄(x±s,岁) 69.32±8.15 65.78±9.02 2.063a 0.041 性别(男性/女性,例) 23/15 45/38 0.418b 0.524 高血压[例(%)] 28(73.7) 52(62.7) 1.405b 0.236 糖尿病[例(%)] 15(39.5) 22(26.5) 2.048b 0.152 吸烟史[例(%)] 18(47.4) 30(36.1) 1.361b 0.243 房颤[例(%)] 10(26.3) 15(18.1) 1.072b 0.301 高脂血症[例(%)] 22(57.9) 38(45.8) 1.517b 0.218 冠心病[例(%)] 12(31.6) 18(21.7) 1.357b 0.244 病变部位(前循环/后循环,例) 25/13 60/23 0.523b 0.470 入院时NIHSS评分(x±s,分) 9.21±2.89 6.85±3.12 4.502a < 0.001 mRS评分[M(P25, P75),分] 3(2,3) 2(2,3) 1.035c 0.297 LDL-C(x±s,mmol/L) 3.42±0.87 2.85±0.79 3.568a 0.001 HbA1c(x±s,%) 6.35±1.23 5.78±1.09 2.563a 0.012 总胆固醇(x±s,mmol/L) 5.17±1.12 4.52±1.05 3.095a 0.002 甘油三酯(x±s,mmol/L) 1.68±0.75 1.52±0.68 1.163a 0.247 HDL-C(x±s,mmol/L) 1.12±0.28 1.05±0.25 1.376a 0.171 空腹血糖(x±s,mmol/L) 6.54±1.87 6.12±1.72 1.213a 0.228 脑钠肽(x±s,pg/mL) 115.23±48.51 108.68±42.33 0.749a 0.455 C反应蛋白[M(P25, P75),mg/L] 9.96(3.61, 12.98) 8.81(2.83, 11.47) -0.754c 0.451 Hcy(x±s,μmol/L) 13.18±4.77 12.52±4.23 0.813a 0.418 注:a为t值,b为χ2值,c为Z值。  下载: 导出CSV
下载: 导出CSV
表 2 2组AIS患者血清TSPO、BDNF和TNF-α水平比较(x±s)
Table 2. Comparison of serum TSPO, BDNF and TNF-α levels between the two groups of AIS patients (x±s)
组别 例数 TSPO (ng/mL) BDNF (ng/mL) TNF-α (pg/mL) PSD组 38 3.25±1.08 10.52±3.65 7.85±2.12 非PSD组 83 2.78±0.95 12.85±4.12 6.92±1.85 t值 2.418 2.989 2.450 P值 0.017 0.003 0.016
下载: 导出CSV
表 3 AIS患者PSD发生影响因素的单因素logistic回归分析
Table 3. Single factor and logistic regression analysis of the influencing factors of PSD occurrence of AIS patients
变量 B SE Waldχ2 P值 OR值 95% CI 年龄 0.064 0.029 4.870 0.039 1.066 1.003~1.133 性别 0.218 0.412 0.280 0.542 1.243 0.601~2.572 高血压 0.445 0.387 1.322 0.221 1.560 0.764~3.186 糖尿病 0.871 0.401 4.718 0.028 2.389 1.098~5.198 吸烟史 0.405 0.381 1.130 0.273 1.500 0.721~3.121 房颤 0.367 0.581 0.399 0.401 1.443 0.598~3.484 高脂血症 0.647 0.354 3.340 0.085 1.910 0.914~4.000 冠心病 0.521 0.368 2.004 0.215 1.684 0.742~3.810 病变部位 -0.255 0.378 0.455 0.498 0.775 0.374~1.605 入院时NIHSS评分 0.279 0.084 11.032 0.003 1.310 1.098~1.565 总胆固醇 0.398 0.283 1.978 0.053 1.489 0.996~2.222 甘油三酯 0.357 0.251 2.023 0.203 1.429 0.821~2.486 HDL-C 0.562 0.321 3.065 0.151 1.754 0.818~3.761 LDL-C 0.511 0.231 4.893 0.027 1.667 1.001~2.777 空腹血糖 0.176 0.111 2.514 0.136 1.192 0.981~1.448 HbA1c 0.385 0.176 4.785 0.029 1.470 1.041~2.075 TSPO 0.832 0.357 5.431 0.020 2.298 1.141~4.626 BDNF -0.427 0.163 6.862 0.009 0.652 0.474~0.898 TNF-α 0.402 0.189 4.524 0.033 1.495 1.032~2.165 注:变量赋值如下,女性=0,男性=1;高血压、糖尿病、吸烟史、房颤、高脂血症、冠心病、赋值均为是=1,否=0;病变部位为前循环=1,后循环=0;其他变量为连续变量,均以实际值赋值。
下载: 导出CSV
表 4 AIS患者PSD发生影响因素的多因素logistic回归分析
Table 4. Multi-factor and logistic regression analysis of the influencing factors of PSD occurrence of AIS patients
变量 B SE Waldχ2 P值 OR值 95% CI 年龄 0.087 0.049 3.152 0.076 1.091 0.991~1.201 糖尿病 0.918 0.426 4.644 0.035 2.504 1.087~5.832 入院时NIHSS评分 0.241 0.088 7.540 0.006 1.273 1.071~1.514 LDL-C 0.583 0.251 5.395 0.020 1.792 1.078~2.978 HbA1c 0.431 0.191 5.092 0.019 1.539 1.091~2.174 TSPO 0.725 0.341 4.531 0.035 2.065 1.052~4.055 BDNF -0.362 0.157 5.316 0.011 0.696 0.521~0.929 TNF-α 0.318 0.148 4.617 0.036 1.374 1.031~1.832
下载: 导出CSV
表 5 血清TSPO、BDNF和TNF-α预测AIS患者发生PSD的临床效能
Table 5. Clinical efficacy of serum TSPO, BDNF and TNF-α in predicting PSD of AIS patients
项目 SE AUC 95% CI 最佳临界值 灵敏度(%) 特异度(%) 约登指数 TSPO 0.055 0.684 0.593~0.765 3.00 ng/mL 71.05 65.06 0.36 BDNF 0.053 0.666 0.574~0.749 11.15 ng/mL 57.89 69.88 0.38 TNF-α 0.053 0.687 0.581~0.773 7.01 pg/mL 73.55 63.86 0.36 三者联合 0.044 0.797 0.715~0.865 82.72 75.93 0.57
下载: 导出CSV
-
[1] GUO J L, WANG J J, SUN W, et al. The advances of post-stroke depression: 2021 update[J]. J Neurol, 2022, 269(3): 1236-1249. doi: 10.1007/s00415-021-10597-4 [2] JING D Q, HOU X L, GUO X, et al. Astrocytes in post-stroke depression: roles in inflammation, neurotransmission, and neurotrophin signaling[J]. Cell Mol Neurobiol, 2023, 43(7): 3301-3313. doi: 10.1007/s10571-023-01386-w [3] SUN N, CUI W Q, MIN X M, et al. A new perspective on hippocampal synaptic plasticity and post-stroke depression[J]. Eur J Neurosci, 2023, 58(4): 2961-2984. doi: 10.1111/ejn.16093 [4] CONTI E, GRANA D, ANGIULLI F, et al. TSPO modulates oligomeric amyloid-β-induced monocyte chemotaxis: relevance for neuroinflammation in Alzheimer's disease[J]. J Alzheimers Dis, 2023, 95(2): 549-559. doi: 10.3233/JAD-230239 [5] MAHEMUTI Y, KADEER K, SU R, et al. TSPO exacerbates acute cerebral ischemia/reperfusion injury by inducing autophagy dysfunction[J]. Exp Neurol, 2023, 369: 114542. DOI: 10.1016/j.expneurol.2023.114542. [6] DU X C, CHEN W, ZHAN N, et al. The effects of low-intensity resistance training with or without blood flow restriction on serum BDNF, VEGF and perception in patients with post-stroke depression[J]. Neuro Endocrinol Lett, 2021, 42(4): 229-235. [7] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-682.Chinese Society of Neurology, Cerebrovascular Group, Chinese Society of Neurology. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018[J]. Chinese Journal of Neurology, 2018, 51(9): 666-682. [8] HENDRIX P, MELAMED I, COLLINS M, et al. NIHSS 24 h after mechanical thrombectomy predicts 90-day functional outcome[J]. Clin Neuroradiol, 2022, 32(2): 401-406. doi: 10.1007/s00062-021-01068-4 [9] KRIEGER P, MELMED K R, TORRES J, et al. Pre-admission antithrombotic use is associated with 3-month mRS score after thrombectomy for acute ischemic stroke[J]. J Thromb Thrombolysis, 2022, 54(2): 350-359. doi: 10.1007/s11239-022-02680-y [10] JIAO Q Y, DONG Y Q, MA X J, et al. Does baseline cognitive function predict the reduction rate in HRDS-17 total scores in first-episode, drug-naïve patients with major depressive disorder?[J]. Neuropsychiatr Dis Treat, 2024, 20: 353-361. doi: 10.2147/NDT.S453447 [11] GARLAND E F, DENNETT O, LAU L C, et al. The mitochondrial protein TSPO in Alzheimer's disease: relation to the severity of AD pathology and the neuroinflammatory environment[J]. J Neuroinflammation, 2023, 20(1): 186. DOI: 10.1186/s12974-023-02869-9. [12] 郭蔚虹, 孙琼其, 陈瑞娟. 创伤性脑损伤患者血清IL-1β, MMP-9及TSPO水平与疾病程度及预后评估的价值研究[J]. 现代检验医学杂志, 2021, 36(6): 162-165.GUO W H, SUN Q Q, CHEN R J. Value of levels of serum IL-1 β, MMP-9 and TSPO in evaluating the severity and prognosis of traumatic brain injury[J]. Journal of Modern Laboratory Medicine, 2021, 36(6): 162-165. [13] 瞿慧, 张霞, 梁朝明, 等. 血清TSPO、Nesfatin-1、AngⅡ与产后抑郁症的关系分析及其预测价值研究[J]. 现代生物医学进展, 2023, 23(12): 2387-2391.QU H, ZHANG X, LIANG C M, et al. Analysis of relationship between serum TSPO, Nesfatin-1, Ang Ⅱand postpartum depression and their predictive value study[J]. Progress in Modern Biomedicine, 2023, 23(12): 2387-2391. [14] RUPPRECHT R, PRADHAN A K, KUFNER M, et al. Neurosteroids and translocator protein 18 kDa (TSPO) in depression: implications for synaptic plasticity, cognition, and treatment options[J]. Eur Arch Psychiatry Clin Neurosci, 2023, 273(7): 1477-1487. doi: 10.1007/s00406-022-01532-3 [15] RIEBEL M, BRUNNER L M, NOTHDURFTER C, et al. Neurosteroids and translocator protein 18 kDa (TSPO) ligands as novel treatment options in depression[J]. Eur Arch Psychiatry Clin Neurosci, 2024. DOI: 10.1007/s00406-024-01843-7. [16] 焦爱菊, 任宝龙, 张春花, 等. NIHSS评分联合血清BDNF、IL-6对脑卒中后抑郁的预测价值[J]. 天津医药, 2024, 52(9): 963-966.JIAO A J, REN B L, ZHANG C H, et al. The predictive value of NIHSS score combined with serum BDNF and IL-6 for post-stroke depression[J]. Tianjin Medical Journal, 2024, 52(9): 963-966. [17] 毛亚娣, 孙剑虹, 刘蓝冰, 等. 生物波穴位刺激联合中医情志护理对脑卒中后抑郁患者恢复效果的影响[J]. 中华全科医学, 2023, 21(3): 530-533. doi: 10.16766/j.cnki.issn.1674-4152.002924MAO Y D, SUN J H, LIU L B, et al. Effect of bio-wave acupoint stimulation combined with emotional nursing of traditional Chinese medicine on recovery in patients with post-stroke depression[J]. Chinese Journal of General Practice, 2023, 21(3): 530-533. doi: 10.16766/j.cnki.issn.1674-4152.002924 [18] JIN Y H, YU L M, LI Y. Paroxetine effect on nerve growth factor, human neurotrophin-4, brain-derived neurotrophic factor levels in post-stroke depression[J]. Mol Neurobiol, 2024, 61(10): 7890-7897. doi: 10.1007/s12035-024-04084-w [19] 黄能, 刘祚燕, 屈云. 不同年龄脑卒中患者出院后六个月康复状况的调查研究[J]. 华西医学, 2022, 37(1): 56-61.HUANG N, LIU Z Y, QU Y. Investigation on the rehabilitation status of patients with cerebral apoplexy at different ages six months after discharge from hospital[J]. West China Medical Journal, 2022, 37(1): 56-61. [20] BIANCIARDI E, BARONE Y, LO SERRO V, et al. Inflammatory markers of perinatal depression in women with and without history of trauma[J]. Riv Psichiatr, 2021, 56(5): 237-245. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 10
- HTML全文浏览量: 3
- PDF下载量: 0
- 被引次数: 0
