

Analysis of risk factors affecting all-cause mortality in patients with coronary artery disease with mitral regurgitation
-
摘要:
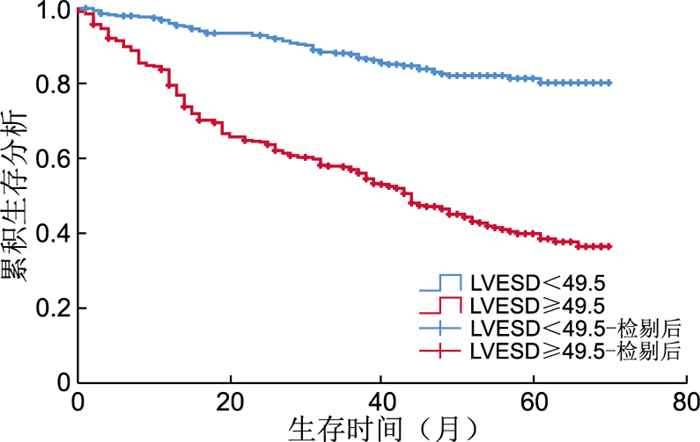
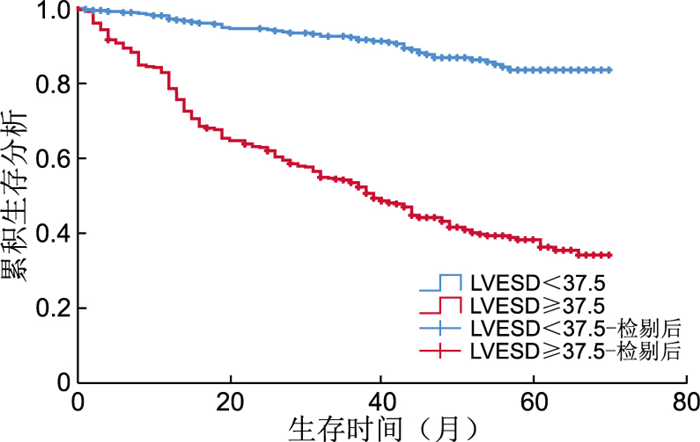
目的 冠心病(CAD)发病率持续上升,二尖瓣反流(MR)是最常见的心脏瓣膜疾病,本研究旨在探讨冠心病伴MR患者的临床特征,分析影响预后的危险因素。 方法 本研究纳入2018年1月—2023年12月在新疆维吾尔自治区人民医院住院时诊断为冠心病且伴有二尖瓣反流的813例患者,中位随访时间为2.5年,以全因死亡为终点事件,根据是否发生终点事件将患者分为终点事件组(314例)和非终点事件组(499例)。采用Cox回归分析研究影响患者预后的因素。通过ROC曲线评估左房内径(LAD)、左室舒张期末内径(LVEDD)、左室收缩期末内径(LVESD)对预后的预测能力,并根据Youden指数确定最佳截断值,利用Kaplan-Meier生存曲线分析生存情况。 结果 变量校正后,LAD(HR=1.031,95% CI:1.015~1.048)、LVEDD(HR=1.057,95% CI:1.043~1.071)、LVESD(HR=1.046,95% CI:1.031~1.062)增大均是冠心病伴MR患者发生终点事件的危险因素(P < 0.001)。ROC曲线显示,LAD、LVEDD、LVESD对冠心病伴MR患者远期全因死亡具有预测能力(AUC分别为0.666、0.755、0.761,P<0.001),最佳截断值分别为42.5 mm、49.5 mm、37.5 mm;Kaplan-Meier生存曲线显示,超过上述阈值者生存率显著降低(log-rank χ2=59.737、123.156、171.803,P<0.001)。 结论 心脏超声心动图指标对冠心病伴二尖瓣反流患者预后有预测价值,其中LAD、LVEDD、LVESD增大是患者发生终点事件的危险因素。 Abstract:Objective The incidence of coronary artery disease (CAD) continues to increase, and mitral regurgitation (MR) is the most common heart valve disease. This study aims to investigate the clinical characteristics exhibited by patients diagnosed with coronary artery disease with MR and analyze the risk factors that have a detrimental effect on their prognosis. Methods This study comprised 813 patients diagnosed with coronary artery disease with mitral regurgitation, who were admitted to the Xinjiang Uygur Autonomous Region People's Hospital from January 2018 to December 2023, with a median follow-up period of 2.5 years, and the primary focus of the analysis was all-cause mortality. Patients were categorized into an endpoint event group (n=314) and a non-endpoint event group (n=499) according to the occurrence of an endpoint event. A Cox regression model was used to analyze the correlation between echocardiographic indices and prognosis in the present study, and the predictive ability of left atrial diameter (LAD), left ventricular end-diastolic internal diameter (LVEDD), and left ventricular end-systolic internal diameter (LVESD) for prognosis was assessed by the subjects' operating curves (ROCs), and the optimal cut-off values were determined by the Youden index, and analyzed by using the Kaplan-Meier survival curve. Results After making several adjustments to the data, it was found that LAD (HR=1.031, 95% CI: 1.015-1.048), LVEDD (HR=1.057, 95% CI: 1.043-1.071), LVESD (HR=1.046, 95% CI: 1.031-1.062) were all risk factors for the occurrence of endpoint events in patients with coronary heart disease and MR (P < 0.001). The ROC curve showed that LAD, LVEDD and LVESD could predict long-term all-cause death in patients with coronary heart disease and MR (AUC=0.666, 0.755, 0.761, P < 0.001), and the best cut-off values were 42.5 mm, 49.5 mm and 37.5 mm, respectively. The Kaplan-Meier survival curve showed that the survival rate of patients above the threshold was significantly reduced (log-rank χ2=59.737, 123.156, 171.803, P < 0.001). Conclusion Cardiac echocardiographic indices have been shown to possess a degree of predictive value regarding prognosis in patients suffering from coronary artery disease and mitral regurgitation, and the increase of LAD, LVEDD and LVESD has been identified as a risk factor for endpoint events in patients. -

图 1 LAD、LVEDD、LVESD预测CAD-MR患者预后的ROC曲线
Figure 1. ROC curves of LAD, LVEDD, and LVESD for predicting the prognosis of patients with CAD-MR

图 2 LAD≥42.5 mm时CAD-MR患者全因死亡K-M曲线
Figure 2. K-M curve for all-cause mortality in CAD-MR patients with LAD≥42.5 mm

图 3 LVEDD≥49.5 mm时CAD-MR患者全因死亡K-M曲线
Figure 3. K-M curve for all-cause mortality in CAD-MR patients with LVEDD≥49.5 mm

图 4 LVESD≥37.5 mm时CAD-MR患者全因死亡K-M曲线
Figure 4. K-M curve for all-cause mortality in CAD-MR with LVESD ≥37.5 mm
表 1 2组冠心病伴MR患者一般资料比较
Table 1. Comparison of general data between the two groups of CHD patients with MR
项目 终点事件组(n=314) 非终点事件组(n=499) 统计量 P值 年龄[M(P25, P75),岁] 74(65,81) 69(60,77) 5.610a <0.001 性别[例(%)] 0.466b 0.495 男性 185(58.9) 306(61.3) 女性 129(41.1) 193(38.7) 高血压[例(%)] 210(66.9) 346(69.3) 0.539b 0.463 糖尿病[例(%)] 116(36.9) 178(35.7) 0.135b 0.713 吸烟史[例(%)] 74(23.6) 126(25.3) 0.295b 0.587 经皮冠状动脉介入术[例(%)] 92(29.3) 156(31.3) 0.350b 0.554 NYHA Ⅳ级[例(%)] 131(41.7) 117(23.4) 30.355b <0.001 收缩压(x±s,mmHg) 129.35±23.31 131.28±21.90 2.769c 0.006 白细胞(x±s,109/L) 7.20±2.90 7.14±2.66 0.330c 0.741 红细胞[M(P25, P75),109/L] 4.33(3.74,4.79) 4.45(4.01,4.89) 1.246a 0.087 血红蛋白[M(P25, P75),g/L] 127(109,142) 133(120,144) -3.760a <0.001 D-二聚体[M(P25, P75),mg/L] 1.04(0.50,2.03) 0.65(0.35,1.42) 4.639a <0.001 肌酐[M(P25, P75),μmol/L] 84.25(67.25,120.38) 75.90(62.40,97.00) 2.017a 0.044 尿酸[M(P25, P75),μmol/L] 382.82(308.25,492.79) 366.00(289.00,448.84) 3.010a 0.003 注:a为Z值,b为χ2值,c为t值;1 mmHg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 2组冠心病伴MR患者超声指标比较(mm)
Table 2. Comparison of ultrasound parameters between the two groups of patients with coronary heart disease and MR (mm)
组别 例数 RVD
(x±s)PAD
[M(P25, P75)]LAD
[M(P25, P75)]IVS
(x±s)LVEDD
[M(P25, P75)]LVESD
[M(P25, P75)]终点事件组 314 22.12±3.37 21.00(20.00,23.00) 44.00(41.75,47.00) 10.99±1.19 56.00(50.00,64.00) 42.00(39.00,46.00) 非终点事件组 499 21.82±2.66 20.00(20.00,22.00) 42.00(38.00,46.00) 10.96±1.42 48.00(45.00,52.00) 34.00(28.00,41.00) 统计量 1.340a 2.863b 6.452b 0.242a 13.078b 14.145b P值 0.181 0.004 <0.001 0.809 <0.001 <0.001 注:a为t值,b为Z值。
下载: 导出CSV
表 3 预测冠心病伴MR组患者发生终点事件的单因素及多因素Cox回归分析
Table 3. Univariate and multivariate Cox regression analyses predicting the occurrence of endpoint events after 2.5 years of follow-up in the group of patients with coronary artery disease with MR
变量 单因素分析 多因素分析 HR(95% CI) P值 HR(95% CI) P值 年龄 1.023(1.013~1.034) < 0.001 1.037(1.026~1.048) < 0.001 RVD 1.021(0.986~1.058) 0.240 0.958(0.917~1.001) 0.053 PAD 1.048(1.010~1.086) 0.012 0.994(0.947~1.043) 0.795 LAD 1.060(1.045~1.076) < 0.001 1.031(1.015~1.048) < 0.001 IVS 1.011(0.932~1.096) 0.797 1.020(0.937~1.110) 0.646 LVEDD 1.077(1.066~1.089) < 0.001 1.057(1.043~1.071) < 0.001 LVESD 1.069(1.056~1.081) < 0.001 1.046(1.031~1.062) < 0.001
下载: 导出CSV
-
[1] YAN Z S, ZHANG N C, LI K, et al. Upregulation of long non-coding RNA myocardial infarction-associated transcription is correlated with coronary artery stenosis and elevated inflammation in patients with coronary atherosclerotic heart disease[J]. Kaohsiung J Med Sci, 2021, 37(12): 1038-1047. doi: 10.1002/kjm2.12444 [2] 黄万众, 苏强. 冠心病与精神心理疾病的相关性与研究现状[J]. 中华全科医学, 2024, 22(7): 1212-1216.HUANG W Z, SU Q. The correlation and research status of coronary heart disease and psychiatric disorders[J]. Chinese Journal of General Practice, 2024, 22(7): 1212-1216. [3] VAHANIAN A, BEYERSDORF F, PRAZ F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)[J]. Eur Heart J, 2022, 43(7): 561-632. doi: 10.1093/eurheartj/ehab395 [4] 董桂福, 王宇航, 葛建军. 不停跳冠脉搭桥心肌保护技术在瓣膜疾病合并冠心病手术中的应用[J]. 中华全科医学, 2021, 19(10): 1650-1653.DONG G F, WANG Y H, GE J J. Application analysis of myocardial protection technique for off-pump coronary artery bypass grafting in the operation of valve disease combined with coronary heart disease[J]. Chinese Journal of General Practice, 2021, 19(10): 1650-1653. [5] ZEGARD A, OKAFOR O, DE BONO J, et al. Myocardial fibrosis as a predictor of sudden death in patients with coronary artery disease[J]. J Am Coll Cardiol, 2021, 77(1): 29-41. doi: 10.1016/j.jacc.2020.10.046 [6] ARORA S, SIVARAJ K, HENDRICKSON M, et al. Prevalence and prognostic significance of mitral regurgitation in acute decompensated heart failure: the ARIC study[J]. JACC Heart Fail, 2021, 9(3): 179-189. doi: 10.1016/j.jchf.2020.09.015 [7] HARADA T, NASER J A, TADA A, et al. Cardiac function, haemodynamics, and valve competence with exercise in patients with heart failure with preserved ejection fraction and mild to moderate secondary mitral regurgitation[J]. Eur J Heart Fail, 2024, 26(7): 1616-1627. doi: 10.1002/ejhf.3322 [8] COLLET J P, THIELE H, BARBATO E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2021, 42(14): 1289-1367. doi: 10.1093/eurheartj/ehaa575 [9] MARCHETTI D, DI LENARDA F, NOVEMBRE M L, et al. Contemporary echocardiographic evaluation of mitral regurgitation and guidance for percutaneous mitral valve repair[J]. J Clin Med, 2023, 12(22): 7121. DOI: 10.3390/jcm12227121. [10] RETHEMIOTAKI I. Global prevalence of cardiovascular diseases by gender and age during 2010-2019[J]. Arch Med Sci Atheroscler Dis, 2023, 8: e196-e205. [11] O'GARA P T, MACK M J. Secondary mitral regurgitation[J]. N Engl J Med, 2020, 383(15): 1458-1467. doi: 10.1056/NEJMcp1903331 [12] CHEHAB O, ROBERTS-THOMSON R, NG YIN LING C, et al. Secondary mitral regurgitation: pathophysiology, proportionality and prognosis[J]. Heart, 2020, 106(10): 716-723. doi: 10.1136/heartjnl-2019-316238 [13] VON JEINSEN B, SHORT M I, LARSON M G, et al. Prognostic significance of echocardiographic measures of cardiac remodeling[J]. J Am Soc Echocardiogr, 2020, 33(1): 72-81. doi: 10.1016/j.echo.2019.08.001 [14] FERNANDES L P, BARRETO A T F, NETO M G, et al. Prognostic power of conventional echocardiography in individuals without history of cardiovascular diseases: a systematic review and meta-analysis[J]. Clinics (Sao Paulo), 2021, 76: e2754. DOI: 10.6061/clinics/2021/e2754. [15] ZILBERSZAC R, GLEISS A, MASSETTI M, et al. Left atrial size predicts outcome in severe but asymptomatic mitral regurgitation[J]. Sci Rep, 2023, 13(1): 3892. DOI: 10.1038/s41598-023-31163-0. [16] 李雨濛, 吴华芹, 张并璇, 等. 左室舒张末期内径对慢性心力衰竭患者远期预后的预测价值[J]. 中国循证心血管医学杂志, 2022, 14(11): 1341-1344, 1348.LI Y M, WU H Q, ZHANG B X, et al. Predictive value of left ventricular end-diastolic inner diameter to long-term prognosis in patients with chronic heart failure[J]. Chinese Journal of Evidence-Based Cardiovascular Medicine, 2022, 14(11): 1341-1344, 1348. [17] DUGGAN J P, PETERS A S, TRACHIOTIS G D, et al. Epidemiology of coronary artery disease[J]. Surg Clin North Am, 2022, 102(3): 499-516. doi: 10.1016/j.suc.2022.01.007 -


 点击查看大图
点击查看大图

计量
- 文章访问数: 5
- HTML全文浏览量: 2
- PDF下载量: 0
- 被引次数: 0
