

Construction and validation of a malnutrition risk prediction model for patients recovering from stroke
-
摘要:
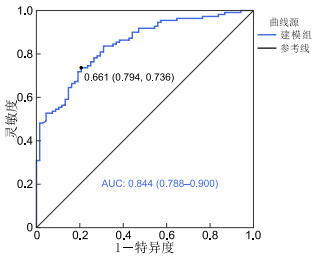
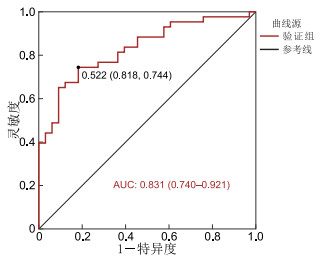
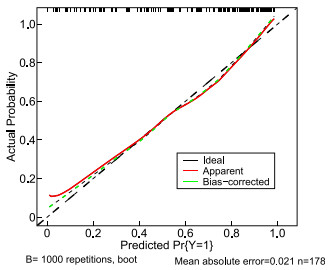
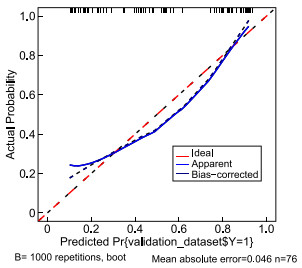
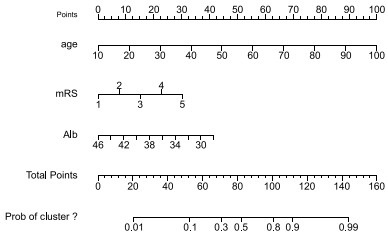
目的 分析脑卒中恢复期患者营养不良的风险因素,构建列线图模型,并验证该模型的预测效果。 方法 选取2021年12月—2022年11月十堰市太和医院254名脑卒中恢复期患者,其中2021年12月—2022年7月的178例作为建模组,2022年8—11月的76例作为验证组。对建模组数据采用单因素分析和logistic回归分析研究脑卒中恢复期患者营养不良的风险因素,构建列线图模型并进行效果验证。 结果 脑卒中恢复期患者营养不良风险发生率为60.24%(153/254),其中建模组与验证组营养不良风险发生率分别为61.80%(110/178)和56.58%(43/76)。年龄(OR=1.086,P<0.001)、改良Rankin量表(mRS)评分(OR=1.756,P=0.001)、ALB水平(OR=0.842,P=0.012)均为脑卒中恢复期患者营养不良的独立影响因素。构建模型为:Logit(P)=0.402+0.083×年龄+0.563×mRS评分-0.172×ALB水平。建模组和验证组模型AUC分别为0.844(95% CI:0.788~0.900)和0.831(95% CI:0.740~0.921)。 结论 年龄越大、mRS评分越高、ALB水平越低,脑卒中恢复期患者营养不良的发生风险越大。本研究构建的风险预测模型具有较好的区分度和校准度,可作为参考工具,便于临床医护人员早期识别脑卒中恢复期患者的营养不良发生风险。 Abstract:Objective Analyzing risk factors for malnutrition in patients recovering from stroke, constructing a nomogram model, and validating its predictive effect. Methods A total of 254 stroke recovery patients were admitted to Taihe hospital in Shiyan City from December 2021 to November 2022. Among them, 178 cases from December 2021 to July 2022 were used as the modeling group, and 76 cases from August to November 2022 were used as the validation group. The data in the modeling group were analyzed using one-way analysis and logistic regression analysis to determine the malnutrition risk factors in patients recovering from stroke. Constructed a column-line diagram model and verified the effect. Results The incidence of malnutrition risk in patients recovering from stroke was 60.24% (153/254). The incidences of malnutrition risk were 61.80% (110/178) and 56.58% (43/76) in the modeling and validation groups, respectively. The age (OR=1.086, P < 0.001), mRS score (OR=1.756, P=0.001), and ALB level (OR=0.842, P=0.012) were independent influencing factors for the risk of malnutrition in patients recovering from stroke. The model was constructed as follows: Logit(P)=0.402+0.083×age+0.563×mRS score-0.172×ALB level. The AUCs of the modeling and validation group models were 0.844 (95% CI: 0.788-0.900) and 0.831 (95% CI: 0.740-0.921), respectively. Conclusion The older the age, the higher the mRS score, and the lower the ALB level, the greater the risk of malnutrition in patients recovering from stroke. This risk prediction model constructed in this study has good discrimination and calibration, and can be used as a reference tool to facilitate early identification of malnutrition risk in patients recovering from stroke by clinical health care professionals. -
Key words:
- Stroke /
- Convalescence /
- Malnutrition /
- Prediction model /
- Nomogram
-
表 1 建模组脑卒中恢复期患者营养不良风险因素的单因素分析
Table 1. Univariate analysis of the risk for malnutrition in patients in the modeling group
项目 合计(n=178) 非营养不良风险组(n=68) 营养不良风险组(n=110) 统计量 P值 年龄(x ±s, 岁) 59.08±11.84 52.41±9.61 63.21±11.22 6.824a <0.001 职业状况[例(%)] 16.406b <0.001 在职 45(25.28) 25(55.56) 20(44.44) 退休 46(25.84) 7(15.22) 39(84.78) 无业 87(48.88) 36(41.38) 51(58.62) 医疗支付类型[例(%)] 4.627b 0.031 城乡居民医保 97(54.49) 44(45.36) 53(54.64) 城镇职工医保 81(45.51) 24(29.63) 57(70.37) 照顾类型[例(%)] 13.729b 0.001 亲属 137(76.97) 49(35.77) 88(64.23) 保姆/护工 30(16.85) 9(30.00) 21(70.00) 无人照顾 11(6.18) 10(90.91) 1(9.09) 发病时间[M(P25, P75), 月] 1.00(1.00, 5.00) 2.00(1.00, 7.75) 1.00(1.00, 3.25) -2.011c 0.044 感染[例(%)] 9.224b 0.002 否 135(75.84) 60(44.44) 75(55.56) 是 43(24.16) 8(18.60) 35(81.40) 吞咽障碍[例(%)] 18.739b <0.001 否 111(62.36) 56(50.45) 55(49.55) 是 67(37.64) 12(17.91) 55(82.09) 服用改善消化道症状药物种类[M(P25, P75), 种] 1.00(0.00, 2.00) 0.00(0.00, 2.00) 1.00(0.00, 2.00) -2.420c 0.016 MBI评分[例(%)] 15.792d <0.001 重度依赖 66(37.08) 13(19.70) 53(80.30) 中度依赖 45(25.28) 21(46.67) 24(53.33) 轻度依赖 54(30.34) 24(44.44) 30(55.56) 无需依赖 13(7.30) 10(76.92) 3(23.08) mRS评分[M(P25, P75), 分] 4.00(2.00, 4.00) 3.00(2.00, 4.00) 4.00(3.00, 4.25) -5.645c <0.001 PSD-S评分(x ±s, 分) 7.64±4.10 6.43±3.96 8.36±4.03 3.137a 0.002 NIHSS评分(x ±s, 分) 7.23±6.50 5.90±9.12 8.05±3.95 2.175a 0.031 进食方式[例(%)] 7.603b 0.006 经口 162(91.01) 67(41.36) 95(58.64) 管饲 16(8.99) 1(6.25) 15(93.75) ALB(x ±s,g/L) 37.94±3.16 39.52±2.87 36.97±2.93 5.687a <0.001 PA(x ±s,g/L) 203.63±51.42 221.25±47.97 192.74±50.66 3.723a <0.001 注:a为t值,b为χ2值,c为Z值,d为H值。本表仅列出差异有统计学意义的项目。  下载: 导出CSV
下载: 导出CSV
表 2 变量赋值情况
Table 2. Table of independent variable assignments
变量 赋值方法 营养不良风险 否=0,是=1 年龄 连续性变量,以实际值赋值 职业状况 在职=(0, 0);退休=(1, 0);无业=(0, 1) 医疗支付类型 城乡居民医保=0,城镇职工医保=1 照顾类型 亲属=(0, 0);保姆/护工=(1, 0);无人照顾=(0, 1) 发病时间 连续性变量,以实际值赋值 合并感染 否=0,是=1 吞咽障碍 否=0,是=0 服用改善消化道药物种类 连续性变量,以实际值赋值 MBI评分 重度依赖=0,中度依赖=1,轻度依赖=2,无需依赖=3 mRS评分 连续性变量,以实际值赋值 PSD-S评分 连续性变量,以实际值赋值 NIHSS评分 连续性变量,以实际值赋值 进食方式 经口=0,管饲=1 ALB 连续性变量,以实际值赋值 PA 连续性变量,以实际值赋值
下载: 导出CSV
表 3 建模组脑卒中恢复期患者营养不良风险因素的多因素分析
Table 3. Multifactorial analysis of the risk for malnutrition in patients in the modeling group
变量 B SE Waldχ2 P值 OR值 95% CI Constant 0.402 3.168 0.016 0.899 1.495 年龄 0.083 0.020 17.353 <0.001 1.086 1.045~1.129 mRS评分 0.563 0.171 10.864 0.001 1.756 1.256~2.454 ALB -0.172 0.068 6.321 0.012 0.842 0.737~0.963 注:本表仅列出差异有统计学意义的变量。
下载: 导出CSV
表 4 建模组与验证组列线图预测价值比较
Table 4. Comparison of prediction effects between modeling and validation groups
组别 灵敏度 特异度 YI 截断值 AUC 95% CI 标准误 P值 建模组 0.736 0.794 0.530 0.661 0.844 0.788~0.900 0.029 <0.001 验证组 0.744 0.818 0.562 0.522 0.831 0.740~0.921 0.046 <0.001
下载: 导出CSV
-
[1] 王陇德, 彭斌, 张鸿祺, 等. 《中国脑卒中防治报告2020》概要[J]. 中国脑血管病杂志, 2022, 19(2): 136-144.WANG L D, PENG B, ZHANG H Q, et al. Brief report on stroke prevention and treatment in China, 2020[J]. Chinese Journal of Cerebrovascular Diseases, 2022, 19(2): 136-144. [2] 李瑞雪, 孙舒, 明巍. 脑卒中患者营养现状分析及筛查方法[J]. 世界最新医学信息文摘, 2019, 19(72): 89-91.LI R X, SUN S, MING W. Analysis of the current nutritional status of stroke patients and screening methods[J]. Word Latest Medicine information, 2019, 19(72): 89-91. [3] ZHANG M, YE S, HUANG X, et al. Comparing the prognostic significance of nutritional screening tools and ESPEN-DCM on 3-month and 12-month outcomes in stroke patients[J]. Clin Nutr, 2021, 40(5): 3346-3353. doi: 10.1016/j.clnu.2020.11.001 [4] NISHIOKA S, OMAGARI K, NISHIOKA E, et al. Concurrent and predictive validity of the mini nutritional assessment short-form and the geriatric nutritional risk index in older stroke rehabilitation patients[J]. J Hum Nutr Diet, 2020, 33(1): 12-22. doi: 10.1111/jhn.12699 [5] 杨辰杰, 陈蕙, 郭淳锋, 等. 去骨瓣减压术后患者颅内感染风险预测模型的构建及验证[J]. 中华全科医学, 2023, 21(9): 1503-1507. doi: 10.16766/j.cnki.issn.1674-4152.003156YANG C J, CHEN H, GUO C F, et al. Construction and validation of a predictive model for the risk of intracranial infection in patients after decompressive craniectomy[J]. Chinese Journal of General Practice, 2023, 21(9): 1503-1507. doi: 10.16766/j.cnki.issn.1674-4152.003156 [6] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国各类主要脑血管病诊断要点2019[J]. 中华神经科杂志, 2019, 52(9): 710-715.Chinese Society of Neurology, Chinese Stroke Society. Diagnostic criteria of cerebrovascular diseases in China (version 2019)[J]. Chinese Journal of Neurology, 2019, 52(9): 710-715. [7] 谢雁鸣, 王永炎. 实用中风病康复学[M]. 北京: 人民卫生出版社, 2010.XIE Y M, WANG Y Y. Practical Stroke Rehabilitation[M]. Beijing: People ' s Health Publishing House, 2010. [8] 孙秀伟, 任海艳, 董敏, 等. 尿路造口周围潮湿相关性皮肤损伤风险预测模型的构建及应用[J]. 军事护理, 2023, 40(1): 40-44.SUN X W, REN H Y, DONG M, et al. Development and Application of A Risk Prediction Model for Peristomal Moisture-Associated Skin Damage[J]. Military Nursing, 2023, 40(1): 40-44. [9] 王小娇, 王宁, 崔宏, 等. 应用老年综合评估技术分析老年脑卒中恢复期病人营养状态的影响因素[J]. 实用老年医学, 2022, 36(8): 809-812.WANG X J, WANG N, CUI H, et al. Analysis of the influencing factors of nutritional status in elderly patients with stroke during convalescence by comprehensive geriatric assessment[J]. Practical Geriatrics, 2022, 36(8): 809-812. [10] KONDRUP J, RASMUSSEN H H, HAMBERG O, et al. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials[J]. Clin Nutr, 2003, 22(3): 321-336. doi: 10.1016/S0261-5614(02)00214-5 [11] SHAH S, VANCLAY F, COOPER B. Improving the sensitivity of the Barthel index for stroke rehabilitation[J]. J Clin Epidemiol, 1989, 42(8): 703-709. doi: 10.1016/0895-4356(89)90065-6 [12] 王赛华, 施加加, 孙莹, 等. 简体版改良Barthel指数在脑卒中恢复期中的信度与效度研究[J]. 中国康复, 2020, 35(4): 179-182.WANG S H, SHI J J, SUN Y, et al. Reliability and validity of the simplified version Modified Barthel Index in convalescence period of stroke[J]. Zhong Guo Kang Fu, 2020, 35(4): 179-182. [13] VAN SWIETEN J C, KOUDSTAAL P J, VISSER M C, et al. Interobserver agreement for the assessment of handicap in stroke patients[J]. Stroke, 1988, 19(5): 604-607. doi: 10.1161/01.STR.19.5.604 [14] 岳莹莹. 卒中后抑郁障碍的评估、诊断标准、风险预测及生物标记物研究[D]. 南京: 东南大学, 2017.YUE Y Y. The study of evaluation, diagnostic criteria, risk prediction, and biomarkers for post-stroke depression[D]. Nanjing: Southeast University, 2017. [15] BROTT T, ADAMS H J, OLINGER C P, et al. Measurements of acute cerebral infarction: a clinical examination scale[J]. Stroke, 1989, 20(7): 864-870. doi: 10.1161/01.STR.20.7.864 [16] HUPPERTZ V, GUIDA S, HOLDOWAY A, et al. Impaired nutritional condition after stroke from the hyperacute to the chronic phase: a systematic review and meta-analysis[J]. Front Neurol, 2022, 12: 780080. DOI: 10.3389/fneur.2021.780080. [17] CHEN X, LI D, LIU Y, et al. Nutritional risk screening 2002 scale and subsequent risk of stroke-associated infection in ischemic stroke: the REMISE study[J]. Front Nutr, 2022, 9: 895803. DOI: 10.3389/fnut.2022.895803. [18] TSUTSUMIUCHI K, WAKABAYASHI H, MAEDA K, et al. Impact of malnutrition on post-stroke cognitive impairment in convalescent rehabilitation ward inpatients[J]. Eur Geriatr Med, 2021, 12(1): 167-174. doi: 10.1007/s41999-020-00393-0 [19] CIANCARELLI I, MORONE G, IOSA M, et al. Influence of oxidative stress and inflammation on nutritional status and neural plasticity: new perspectives on post-stroke neurorehabilitative outcome[J]. Nutrients, 2022, 15(1): 108. DOI: 10.3390/nu15010108. [20] MAHMOUDINEZHAD M, KHALILI M, REZAEEMANESH N, et al. Subjective global assessment of malnutrition and dysphagia effect on the clinical and para-clinical outcomes in elderly ischemic stroke patients: a community-based study[J]. BMC Neurol, 2021, 21(1): 466. DOI: 10.1186/s12883-021-02501-4. [21] HAN X, CAI J, LI Y, et al. Baseline objective malnutritional indices as immune-nutritional predictors of long-term recurrence in patients with acute ischemic stroke[J]. Nutrients, 2022, 14(7): 1337. DOI: 10.3390/nu14071337. [22] 赵诗琦, 王书, 张颖, 等. 老年肺部耐碳青霉烯肠杆菌感染风险预测模型的构建和验证[J]. 中华全科医学, 2023, 21(11): 1860-1864, 1945. doi: 10.16766/j.cnki.issn.1674-4152.003243ZHAO S Q, WANG S, ZHANG Y, et al. Establishment and validation of model for the risk of Carbapenem-Resistant Enterobacteriaceae infection in elderly patients with pulmonary infection[J]. Chinese Journal of General Practice, 2023, 21(11): 1860-1864, 1945. doi: 10.16766/j.cnki.issn.1674-4152.003243 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 15
- HTML全文浏览量: 5
- PDF下载量: 0
- 被引次数: 0
