

Effect of atherosclerotic plaque characteristics of middle cerebral artery on cerebral infarction caused by arterial stenosis
-
摘要:
目的 通过分析高分辨率磁共振血管壁成像(HRMR-VWI)和弥散加权成像(DWI),探讨大脑中动脉(MCA)粥样硬化狭窄患者血管壁特征和梗死模式之间的关系。 方法 回顾性纳入2021年1月—2022年12月连续就诊于郑州大学人民医院的大脑中动脉粥样硬化性疾病导致的急性缺血性卒中患者68例。采用HRMR-VWI获取患者血管壁特征, 根据DWI将患者分为单发脑梗死组和多发脑梗死组,比较2组的动脉粥样硬化危险因素、管腔狭窄程度、斑块特征。采用logistic回归分析研究MCA粥样硬化狭窄患者血管壁特征和梗死模式之间的关系。 结果 68例MCA粥样硬化狭窄患者中,多发脑梗死45例(66.18%),单发脑梗死23例(33.82%)。2组患者的年龄、性别、高血压、糖尿病、高脂血症、吸烟史、心血管疾病史、脑血管疾病史、NIHSS评分等危险因素比较,差异均无统计学意义(P>0.05)。多发脑梗死组狭窄程度及斑块内出血(IPH)发生率均显著高于单发脑梗死组(狭窄程度:P=0.029;IPH:P=0.025)。2组在偏心性、斑块强化等方面差异均无统计学意义(P>0.05)。在校正年龄、性别、高血压、糖尿病、高脂血症、吸烟史、心血管疾病史、脑血管疾病史、NIHSS评分等混杂因素后,logistic回归分析显示IPH(校正后OR=6.525,95% CI:1.108-38.442,P=0.038)是多发性脑梗死的独立预测因素。 结论 IPH与多发性脑梗死独立相关。HRMR-VWI可能为不同MCA梗死模式的机制提供新的见解。 Abstract:Objective To explore the correlation between vessel wall characteristics and infarction patterns in patients with atherosclerotic stenosis of the middle cerebral artery (MCA) using high-resolution magnetic resonance vessel wall imaging (HRMR-VWI) and diffusion-weighted imaging (DWI). Methods A retrospective study was conducted at the People's Hospital of Zhengzhou University from January 2021 to December 2022, involving 68 patients with acute ischemic stroke in the MCA due to atherosclerotic stenosis. Patients were categorized into single-and multiple-infarct groups based on DWI findings, and various atherosclerosis risk factors, degree of lumen stenosis, and plaque characteristics were compared between the two groups. Logistic regression analysis was performed to assess the relationship between vessel wall properties and infarct patterns in MCA atherosclerotic stenosis patients. Results Among 68 patients with atherosclerotic stenosis in the middle cerebral artery, 45 patients (66.18%) had multiple infarcts, and 23 (33.82%) had single infarcts. There were no significant difference in age, sex, hypertension, diabetes, hyperlipidemia, smoking history, cardiovascular disease history, cerebrovascular disease history and NIHSS score between the two groups (P>0.05). Degree of stenosis and prevalence of intraplaque hemorrhage (IPH) were significantly greater in the multiple-infarction group than those in the single-infarction group (degree of stenosis: P=0.029; IPH: P=0.025). There was no significant difference in eccentricity and plaque enhancement between the two groups (P>0.05). After adjusting for age, sex, hypertension, diabetes, hyperlipidemia, smoking history, cardiovascular disease history, cerebrovascular disease history, NIHSS score and other confounding factors, logistic regression analysis showed that IPH (adjusted OR=6.525, 95% CI: 1.108-38.442, P= 0.038) was independent predictor for multiple infarction. Conclusion IPH is independently associated with multiple infarcts. HRMR-VWI may provide new insight into the mechanisms underlying the different MCA infarction patterns. -

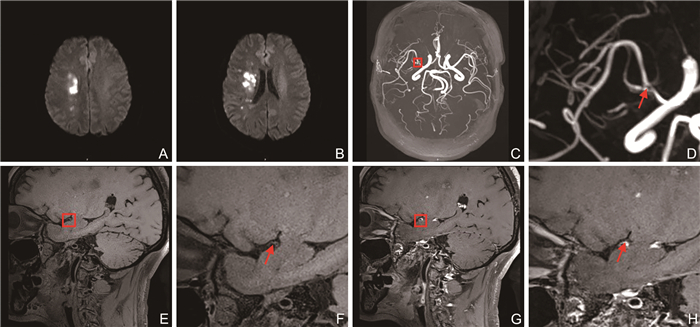
图 1 单发脑梗死患者的HR-MRI特征
注:A、B为DWI序列可见右侧放射冠区及基底节区高信号;C、D为3D-TOF-MRA序列可见右侧MCA M1段纤细狭窄;E、F为T1WI序列可见增厚管壁内膜呈稍长T1信号;G、H为增强T1WI序列可见最狭窄处管壁内膜偏心性轻度强化。
Figure 1. HR-MRI features of patients with single cerebral infarction

图 2 多发脑梗死患者的HR-MRI特征
注:A、B为DWI序列可见右侧额颞顶岛叶、半卵圆中心-放射冠及基底节区多发斑片状、结节状、斑点状高信号;C、D为3D-TOF-MRA序列可见右侧MCA M1段纤细狭窄;E、F为T1WI序列可见增厚管壁内膜呈稍长T1信号;G、H为增强T1WI序列可见狭窄处管壁偏心性轻度强化。
Figure 2. HR-MRI features of patients with multiple cerebral infarction
表 1 单发脑梗死组与多发脑梗死组患者一般资料比较
Table 1. Comparison of general data between single cerebral infarction group and multiple cerebral infarction group
组别 例数 年龄(x±s,岁) 性别(男/女,例) 高血压[例(%)] 糖尿病[例(%)] 高脂血症[例(%)] 吸烟史[例(%)] 心血管疾病史[例(%)] 脑血管疾病史[例(%)] NIHSS评分[M(P25, P75),分] 单发脑梗死组 23 61.96±10.32 15/8 12(52.17) 5(21.74) 2(8.70) 6(26.09) 1(4.35) 2(8.70) 4(3,9) 多发脑梗死组 45 62.18±12.46 25/20 23(51.11) 13(28.89) 8(17.78) 21(46.67) 5(11.11) 7(15.56) 6(4,10) 统计量 0.073a 0.851b 0.009b 0.455b 0.470b 3.237b 0.257b 0.202b -1.947c P值 0.942 0.356 0.923 0.500 0.493 0.072 0.612 0.653 0.052 注:a为t值,b为χ2值,c为Z值。  下载: 导出CSV
下载: 导出CSV
表 2 单发脑梗死组和多发脑梗死组的HR-MRI特征比较
Table 2. Comparison of HR-MRI features between single cerebral infarction group and multiple cerebral infarction group
组别 例数 IPH[例(%)] 偏心性斑块[例(%)] 斑块强化[例(%)] 狭窄程度[M(P25, P75), %] 单发脑梗死组 23 3(13.04) 10(43.48) 20(86.96) 66(58,71) 多发脑梗死组 45 17(37.78) 26(57.78) 41(91.11) 69(65,78) 统计量 5.046a 1.651a 0.162a -2.177b P值 0.025 0.199 0.687 0.029 注:a为χ2值,b为Z值。
下载: 导出CSV
表 3 自变量赋值情况
Table 3. Description of independent variables
自变量 赋值方法 性别 女性=0,男性=1 高血压 无=0,有=1 糖尿病 无=0,有=1 高脂血症 无=0,有=1 吸烟史 无=0,有=1 心血管疾病史 无=0,有=1 脑血管疾病史 无=0,有=1 IPH 无=0,有=1 偏心性斑块 无=0,有=1 斑块强化 无=0,有=1
下载: 导出CSV
表 4 多发性脑梗死预测因素的logistic回归分析
Table 4. Logistic regression analysis of predictive factors of multiple cerebral infarction
预测因素 B SE Waldχ2 P值 OR(95% CI) IPH 1.876 0.905 4.297 0.038 6.525(1.108~38.442) 偏心性斑块 0.673 0.677 0.990 0.320 1.961(0.520~7.388) 斑块强化 0.220 0.957 0.053 0.818 1.247(0.191~8.133) 狭窄程度 0.072 0.038 3.635 0.057 1.075(0.998~1.158) 注:校正年龄、性别、高血压、糖尿病、高脂血症、吸烟史、心血管疾病史、脑血管疾病史、NIHSS评分。
下载: 导出CSV
-
[1] GUTIERREZ J, TURAN T N, HOH B L, et al. Intracranial atherosclerotic stenosis: risk factors, diagnosis, and treatment[J]. Lancet Neurol, 2022, 21(4): 355-368. doi: 10.1016/S1474-4422(21)00376-8 [2] LIANG W B, YIN J Q, LU C Y, et al. Endovascular re-canalization for symptomatic non-acute intracranial large artery occlusion: a single-center retrospective study[J]. Quant Imaging Med Surg, 2023, 13(12): 8031-8041. doi: 10.21037/qims-23-643 [3] FAKIH R, ROA J A, BATHLA G, et al. Detection and quantification of symptomatic atherosclerotic plaques with high-resolution imaging in cryptogenic stroke[J]. Stroke, 2020, 51(12): 3623-3631. doi: 10.1161/STROKEAHA.120.031167 [4] PRABHAKARAN S, LIEBESKIND D S, COTSONIS G, et al. Predictors of early infarct recurrence in patients with symptomatic intracranial atherosclerotic disease[J]. Stroke, 2021, 52(6): 1961-1966. doi: 10.1161/STROKEAHA.120.032676 [5] JING J, MENG X, ZHAO X Q, et al. Dual antiplatelet therapy in transient ischemic attack and minor stroke with different infarction patterns: subgroup analysis of the CHANCE randomized clinical trial[J]. JAMA Neurol, 2018, 75(6): 711-719. doi: 10.1001/jamaneurol.2018.0247 [6] 彭斌, 吴波. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-682. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004PENG B, WU B. Chinese Guidelines for Diagnosis and Treatment of acute ischemic Stroke 2018[J]. Chinese Journal of Neurology, 2018, 51(9): 666-682. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004 [7] DEL BRUTTO V J, CHATURVEDI S, DIENER H C, et al. Antithrombotic therapy to prevent recurrent strokes in ischemic cerebrovascular disease: JACC scientific expert panel[J]. J Am Coll Cardiol, 2019, 74(6): 786-803. doi: 10.1016/j.jacc.2019.06.039 [8] ALMALLOUHI E, NELSON A M, COTSONIS G, et al. Ameliorating racial disparities in vascular risk factor management with aggressive medical management in the SAMMPRIS trial[J]. Stroke, 2023, 54(9): 2235-2240. doi: 10.1161/STROKEAHA.122.042055 [9] 宋明慧, 岳云龙, 郭劲松, 等. MRI 3D SNAP序列对大脑中动脉斑块内出血的研究[J]. 中国医学影像学杂志, 2021, 29(2): 131-135. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYYZ202102009.htmSONG M H, YUE Y L, GUO J S, et al. Three-dimentional simultaneous noncontrast angiography and intraplaque hemorrhage imaging sequence of MRI in the intraplaque hemorrhage of atherosclerotic middle cerebral artery[J]. Chinese Journal of Medical Imaging, 2021, 29(2): 131-135. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYYZ202102009.htm [10] CROMBAG G A J C, SCHREUDER F H B M, VAN HOOF R H M, et al. Microvasculature and intraplaque hemorrhage in atherosclerotic carotid lesions: a cardiovascular magnetic resonance imaging study[J]. J Cardiovasc Magn Reson, 2019, 21(1): 15. doi: 10.1186/s12968-019-0524-9 [11] 孙钦峰, 刘莹, 钱菊, 等. 椎动脉斑块内出血引起反复后循环缺血性脑卒中1例报道[J]. 神经损伤与功能重建, 2023, 18(5): 307-310. https://www.cnki.com.cn/Article/CJFDTOTAL-GWKF202305014.htmSUN Q F, LIU Y, QIAN J, et al. One case of recurrent posterior circulation ischemic stroke caused by intravertebral artery plaque hemorrhage was reported[J]. Neural Injury and Functional Reconstruction, 2023, 18(5): 307-310. https://www.cnki.com.cn/Article/CJFDTOTAL-GWKF202305014.htm [12] LIBBY P. The changing landscape of atherosclerosis[J]. Nature, 2021, 592(7855): 524-533. doi: 10.1038/s41586-021-03392-8 [13] WU F, SONG H Q, MA Q F, et al. Hyperintense plaque on intracranial Vessel Wall magnetic resonance imaging as a predictor of artery-to-artery embolic infarction[J]. Stroke, 2018, 49(4): 905-911. doi: 10.1161/STROKEAHA.117.020046 [14] 田雪, 黄柳, 姚菁青, 等. 血清脂蛋白相关磷脂酶A2水平与颈动脉粥样硬化斑块的相关性分析[J]. 中华全科医学, 2022, 20(11): 1848-1851. doi: 10.16766/j.cnki.issn.1674-4152.002717TIAN X, HUANG L, YAO J Q, et al. Correlation analysis between serum Lp-PLA2 level and carotid atherosclerotic plaque[J]. Chinese Journal of General Practice, 2022, 20(11): 1848-1851. doi: 10.16766/j.cnki.issn.1674-4152.002717 [15] ZHANG N, LYU J H, REN L J, et al. Arterial culprit plaque characteristics revealed by magnetic resonance Vessel Wall imaging in patients with single or multiple infarcts[J]. Magn Reson Imaging, 2021, 84: 12-17. doi: 10.1016/j.mri.2020.06.004 [16] SUN B B, WANG L L, LI X, et al. Intracranial atherosclerotic plaque characteristics and burden associated with recurrent acute stroke: a 3D quantitative Vessel Wall MRI study[J]. Front Aging Neurosci, 2021, 13: 706544. DOI: 10.3389/fnagi.2021.706544. [17] SHI Z, LI J, ZHAO M, et al. Progression of plaque burden of intracranial atherosclerotic plaque predicts recurrent stroke/transient ischemic attack: a pilot follow-up study using Higher-Resolution MRI[J]. J Magn Reson Imaging, 2021, 54(2): 560-570. doi: 10.1002/jmri.27561 -

 点击查看大图
点击查看大图

计量
- 文章访问数: 555
- HTML全文浏览量: 264
- PDF下载量: 12
- 被引次数: 0
