

The prognostic value of lymph node ratio in 89 patients with stage ⅢC1p cervical cancer who underwent surgery
-
摘要:
目的 探讨淋巴结比率(LNR) 对2018年国际妇产科联盟(FIGO) ⅢC1p期宫颈癌患者的预后影响。 方法 纳入2014年1月—2017年12月蚌埠医学院第一附属医院妇瘤科收治的89例淋巴结阳性宫颈癌患者,均接受了根治性子宫切除术以及系统性盆腔联合或不联合腹主动脉旁淋巴结切除术。所有患者术后均接受同步放化疗。LNR定义为阳性淋巴结与移除的淋巴结总数的比率。根据LNR将患者分为2组:LNR<0.06(42例)和LNR≥0.06(47例)。LNR的预后价值通过log-rank检验和多变量Cox回归模型进行评估。 结果 中位随访时间为44.6个月(范围为6~115个月),整个队列的5年无病生存(DFS)率为61.6%,5年总生存(OS)率为69.7%。LNR<0.06和LNR≥0.06的5年DFS率分别为65.4%和54.2%(P=0.027)。此外,LNR<0.06和LNR≥0.06的5年OS率分别为82.8%和59.6%(P=0.003)。在多变量分析中,LNR≥0.06与较差的DFS(HR=2.040,95% CI:1.130~3.870,P=0.013)和OS(HR=1.940,95% CI:1.020~3.780,P=0.038)有相关性。 结论 LNR≥0.06可能是ⅢC1p期宫颈癌患者DFS和OS下降的独立预后因素。 Abstract:Objective To investigate the prognostic impact of lymph node ratio (LNR) on 2018 International Federation of Gynaecology and Obstetrics Stage ⅢC1p cervical cancer patients. Methods A total of 89 patients with lymph node-positive cervical cancer from January 2014 to December 2017 in the Oncology Department of the First Affiliated Hospital Bengbu Medical University underwent radical hysterectomy and systematic pelvic lymphadenectomy with or without abdominal aortic dissection. All patients received concurrent chemoradiotherapy. LNR was defined as the ratio of positive lymph nodes to the total number of LNS removed. Patients were divided into 2 groups according to LNR; LNR < 0.06(42 cases) and LNR≥0.06 (47 cases). The prognostic value of LNR was assessed by univariate log-rank test and multivariable Cox regression models. Results The median follow-up was 44.6 months (range, 6-115 months), and the 5-year disease-free survival (DFS) rate for the entire cohort was 61.6%, while the 5-year overall survival (OS) rate was 69.7%. The 5-year DFS rates for LNR < 0.06 and LNR≥0.06 were 65.4% and 54.2%, respectively (P=0.027). Furthermore, the 5-year OS rates for LNR < 0.06 and LNR≥0.06 were 82.8% and 59.6%, respectively (P=0.003). In multivariable analysis, LNR≥0.06 was associated with worse DFS (HR=2.040, 95% CI: 1.130-3.870, P=0.013) and OS (HR=1.940, 95% CI: 1.020-3.780, P=0.038). Conclusion LNR≥0.06 may be an independent prognostic factor for decreased DFS and OS in patients with stage ⅢC1P cervical cancer. -
Key words:
- Cervical cancer /
- Lymph node ratio /
- Stage ⅢC1p /
- Prognostic analysis
-

图 1 不同LNR水平宫颈癌患者DFS比较
Figure 1. Comparison of DFS in cervical cancer patients with different LNR levels

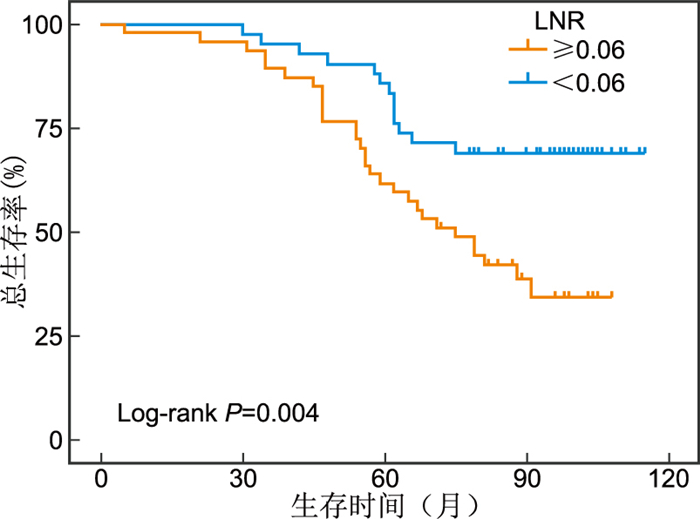
图 2 不同LNR水平宫颈癌患者OS比较
Figure 2. Comparison of OS in cervical cancer patients with different LNR levels
表 1 89例ⅢC1p期宫颈癌患者临床病理特征
Table 1. Clinicopathologic features of 89 cases of cervical cancer with FIGO Stage ⅢC1p in 2018
项目 类别 例数(%) 组织学类型 鳞癌 81(91.0) 非鳞癌 8(9.0) 淋巴脉管间隙受累 阴性 79(88.8) 阳性 10(11.2) 浸润程度 <1/2肌层 15(16.9) ≥1/2肌层 74(83.1) 肿瘤大小 ≤4 cm 58(65.2) >4 cm 31(34.8) 淋巴结比率 <0.06 42(47.2) ≥0.06 47(52.8)  下载: 导出CSV
下载: 导出CSV
表 2 89例ⅢC1p期宫颈癌患者DFS的单因素和多因素分析
Table 2. Univariate and multivariate analysis of DFS in 89 patients with stage Ⅲ C1p cervical cancer
项目 例数 5年DFS[例(%)] 单因素分析P值 多因素分析 HR值 95% CI P值 年龄(岁) 0.680 ≥48 49 24(48.9) <48 40 21(52.5) 组织学类型 <0.001 2.230 1.270~3.830 0.018 鳞癌 81 42(51.8) 非鳞癌 8 3(37.5) 浸润程度 0.860 <1/2肌层 15 8(53.3) ≥1/2肌层 74 37(50.0) 肿瘤大小(cm) 0.010 1.470 0.850~2.790 0.120 ≤4.0 58 36(62.1) >4.0 31 9(29.0) 淋巴脉管间隙受累 0.970 阴性 79 40(50.6) 阳性 10 5(50.0) 淋巴结比率 0.027 2.040 1.130~3.870 0.013 <0.06 42 29(69.0) ≥0.06 47 16(34.0)
下载: 导出CSV
表 3 89例ⅢC1p期宫颈癌患者OS的单因素和多因素分析
Table 3. Univariate and multivariate analysis of OS in 89 patients with stage Ⅲ C1p cervical cancer
项目 例数 5年OS[例(%)] 单因素分析P值 多因素分析 HR值 95% CI P值 年龄(岁) 0.940 ≥48 49 16(32.7) <48 40 11(27.5) 组织学类型 0.020 1.760 0.890~4.120 0.060 鳞癌 81 24(29.6) 非鳞癌 8 3(37.5) 浸润程度 0.890 <1/2肌层 15 5(33.3) ≥1/2肌层 74 22(29.7) 肿瘤大小(cm) 0.038 1.620 0.670~3.130 0.240 ≤4.0 58 23(39.7) >4.0 31 4(12.9) 淋巴脉管间隙受累 0.200 阴性 79 22(27.8) 阳性 10 5(50.0) 淋巴结比率 0.003 1.940 1.020~3.780 0.038 <0.06 42 18(42.9) ≥0.06 47 9(19.1)
下载: 导出CSV
-
[1] WANG M T, MA M, YANG L J, et al. Development and validation of a nomogram for predicting pelvic lymph node metastasis and prognosis in patients with cervical cancer[J]. Front Oncol, 2022, 12: 952347. DOI: 10.3389/fonc.2022.952347. [2] ASLAN K, MEYDANLI M M, OZ M, et al. The prognostic value of lymph node ratio in stage ⅢC cervical cancer patients triaged to primary treatment by radical hysterectomy with systematic pelvic and para-aortic lymphadenectomy[J]. J Gynecol Oncol, 2020, 31(1): e1. DOI: 10.3802/jgo.2020.31.e1. [3] WIDSCHWENDTER P, POLASIK A, JANNI W, et al. Lymph node ratio can better predict prognosis than absolute number of positive lymph nodes in operable cervical carcinoma[J]. Oncol Res Treat, 2020, 43(3): 87-95. doi: 10.1159/000505032 [4] 龙行涛, 周琦, 王冬, 等. 子宫颈癌2018年FIGO新分期ⅢC期患者预后分析[J]. 中国癌症杂志, 2021, 31(8): 725-733. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGAZ202108005.htmLONG X T, ZHOU Q, WANG D, et al. The prognostic value of revised 2018 FIGO stageⅢC in cervical cancer[J]. China Oncology, 2021, 31(8): 725-733. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGAZ202108005.htm [5] RYU J M, CHOI Y S, BAE J Y. Prognostic factors in women with cervical cancer stage ⅢC1r treated with concurrent chemoradiotherapy[J]. J Obstet Gynaecol Res, 2020, 46(7): 1165-1172. doi: 10.1111/jog.14305 [6] FEMANDES A, VIVEROS-CARREÑO D, HOEGL J, et al. Human papillomavirus-independent cervical cancer[J]. Int J Gynecol Cancer, 2022, 32(1): 1-7. doi: 10.1136/ijgc-2021-003014 [7] XU J, MA Y L, MEI H B, et al. Diagnostic value of multimodal magnetic resonance imaging in discriminating between metastatic and non-metastatic pelvic lymph nodes in cervical cancer[J]. Int J Gen Med, 2022, 15: 6279-6288. doi: 10.2147/IJGM.S372154 [8] TOHYAMA A, MURAKAMI M, YOSHINO K. Strategies for the treatment of cervical cancer with bulky pelvic lymph nodes: an overview of the current evidence[J]. J UOEH, 2020, 42(4): 317-325. doi: 10.7888/juoeh.42.317 [9] 张慧慧, 王蓓蓓, 张献文, 等. 伴有盆腔淋巴结转移的宫颈癌新辅助化疗联合放化疗临床疗效及预后因素分析[J]. 中华全科医学, 2021, 19(11): 1823-1826, 1839. doi: 10.16766/j.cnki.issn.1674-4152.002176ZHANG H H, WANG B B, ZHANG X W, et al. Treatment effect and analysis of prognostic factors of neoadjuvant chemotherapy followed by concurrent chemoradiotherapy for advanced cervical cancer with pelvic lymph node metastasis[J]. Chinese Journal of General Practice, 2021, 19(11): 1823-1826, 1839. doi: 10.16766/j.cnki.issn.1674-4152.002176 [10] OLTHOF E P, MOM C H, SNIJDERS M L H, et al. The prognostic value of the number of positive lymph nodes and the lymph node ratio in early-stage cervical cancer[J]. Acta Obstet Gynecol Scand, 2022, 101(5): 550-557. doi: 10.1111/aogs.14316 [11] JIN C, LI J, ZOU C X, et al. Lymph node ratio predicts prognosis in patients with surgically resected invasive pancreatic cystic neoplasms[J]. Transl Cancer Res, 2020, 9(10): 5843-5856. doi: 10.21037/tcr-20-1355 [12] SUPSAMUTCHAI C, WILASRUSMEE C, JIRASIRITHAM J, et al. Recurrence outcome of lymph node ratio in gastric cancer after underwent curative resection: a retrospective cohort study[J]. Ann Med Surg (Lond), 2020, 54: 57-61. doi: 10.1016/j.amsu.2020.04.002 [13] SAKIN A, ALDEMTR M N. Lymph node ratio predicts long-term survival in lymph node-positive breast cancer[J]. Eur J Breast Health, 2020, 16(4): 270-275. doi: 10.5152/ejbh.2020.5809 [14] 余淼, 冉立, 常建英, 等. 淋巴结转移和淋巴结阳性比率对早期宫颈癌预后的影响分析[J]. 中国临床医生杂志, 2020, 48(6): 733-736. doi: 10.3969/j.issn.2095-8552.2020.06.033YU M, RAN L, CHANG J Y, et al. Analysis of the influence of lymph node metastasis and lymph node positive ratio on prognosis of early cervical cancer[J]. Chinese Journal For Clinicians, 2020, 48(6): 733-736. doi: 10.3969/j.issn.2095-8552.2020.06.033 [15] KIM S I, KIM T H, LEE M, et al. Lymph node ratio is a strong prognostic factor in patients with early-stage cervical cancer undergoing minimally invasive radical hysterectomy[J]. Yonsei Med J, 2021, 62(3): 231-239. doi: 10.3349/ymj.2021.62.3.231 [16] BOGANI G, VINTI D, MuRGIA F, et al. Burden of lymphatic disease predicts efficacy of adjuvant radiation and chemotherapy in FIGO 2018 stage ⅢCp cervical cancer[J]. Int J Gynecol Cancer, 2019, 29(9): 1355-1360. doi: 10.1136/ijgc-2019-000669 [17] FAN X, WANG Y F, YANG N, et al. Prognostic analysis of patients with stage ⅢC1p cervical cancer treated by surgery[J]. World J Surg Oncol, 2023, 21(1): 186. doi: 10.1186/s12957-023-03076-9 -

 点击查看大图
点击查看大图

计量
- 文章访问数: 410
- HTML全文浏览量: 209
- PDF下载量: 8
- 被引次数: 0
