

Clinical value of count of circulating tumor cells detection in patients with adenocarcinoma of esophagogastric junction
-
摘要:
目的 研究外周血循环肿瘤细胞(CTCs)计数与食管胃交界腺癌(AEG)患者临床特征和总生存期(OS)的关系,探讨CTCs检测在AEG患者中的临床应用价值。 方法 回顾性分析聊城市人民医院2016年7月—2020年6月收治的154例AEG患者的临床资料,患者治疗前1周均采用阴性富集-荧光原位杂交技术行CTCs检测,分析CTCs计数与患者临床特征及OS的关系。 结果 在早期(Ⅰ~Ⅱ期)AEG患者中,CTCs阳性率为57.1%(32/56),癌胚抗原(CEA)、糖类抗原(CA)19-9、CA72-4的阳性率分别为19.6%(11/56)、1.8%(1/56)、12.5%(7/56)。不同CTCs计数AEG患者脉管内瘤栓(χ2=45.262,P < 0.001)、TNM分期(χ2=14.304,P < 0.001)、淋巴结转移(χ2=5.158,P=0.023)差异均有统计学意义。Log-rank单因素分析提示,CTCs≥2(χ2=12.486,P < 0.001)以及CTCs≥3(χ2=45.344,P < 0.001)与AEG患者OS相关。Cox多因素分析显示,CTCs≥3(HR=2.459,95% CI:1.472~4.107,P=0.001)是AEG患者OS的独立危险因素。 结论 阴性富集-荧光原位杂交技术检测CTCs可作为早期AEG患者的辅助诊断指标,与AEG患者的病理分期以及肿瘤复发转移相关,CTCs≥3可作为AEG患者预后不良的独立危险因素,具有一定的临床应用价值。 Abstract:Objective To investigate the relationship between the count of circulating tumor cells (CTCs) in peripheral blood and the clinical characteristics and overall survival (OS) of patients with adenocarcinoma of esophagogastric junction (AEG), and to explore the clinical application value of CTCs detection in AEG patients. Methods A total of 154 patients with AEG were eligible for enrollment in Liaocheng People ' s Hospital from July 2016 to June 2020 in the retrospective study. Negative enrichment techniques and fluorescence in situ hybridization (NE-FISH) were used to detect CTCs one week before treatment and the relationship between CTCs count and clinical characteristics of AEG patients was then investigated. Moreover, relationship between CTCs count and OS in prognosis were also explored. Results The positive rate of CTCs was 57.1% (32/56) and the positive rates of CEA, CA19-9 and CA72-4 were 19.6% (11/56), 1.8% (1/56) and 12.5% (7/56) respectively in the early AEG patients. The presence of CTCs was significantly correlated with AEG patients, CTCs were positive (≥2) in patients with AEG was significantly correlated with intravascular tumor thrombus (χ2=45.262, P < 0.001), TNM stage (χ2=14.304, P < 0.001)and lymph node metastasis (χ2=5.158, P=0.023). Log-rank univariate analysis showed that CTCs ≥ 2 (χ2=12.486, P < 0.001) and CTCs ≥ 3 (χ2=45.344, P < 0.001) were closely related to OS in AEG patients(P < 0.001). Cox multivariate analysis showed that CTCs ≥ 3 (HR=2.459, 95% CI: 1.472-4.107, P=0.001) was an independent risk factor for the prognosis of OS in AEG patients. Conclusion The detection of CTCs by negative enrichment fluorescence in situ hybridization can be used as an auxiliary diagnostic indicator for early AEG patients, which is closely related to the pathological stage of AEG patients and tumor recurrence and metastasis. CTCs ≥ 3 can be used as an independent risk factor for poor prognosis of AEG patients and have a certain clinical application value. -

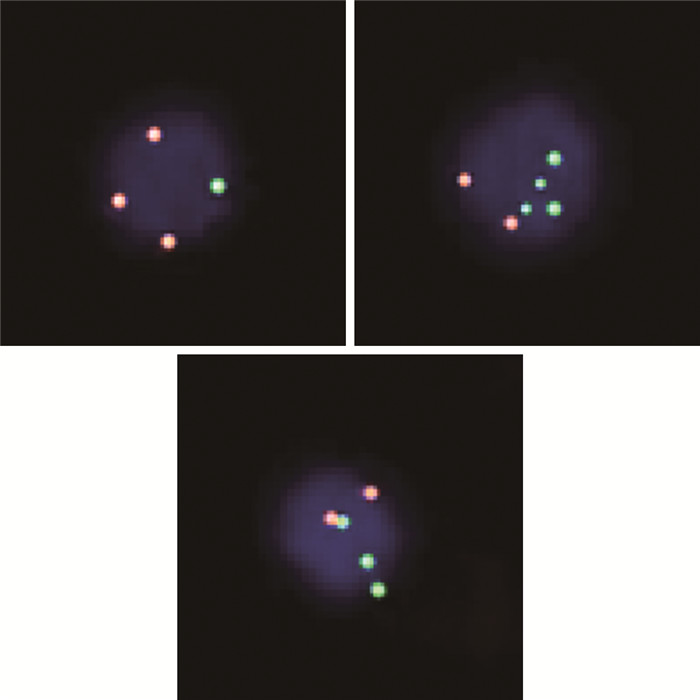
图 1 阴性富集-荧光原位杂交技术检测AEG患者外周血CTCs
Figure 1. Detection of CTCs in the peripheral blood of patients with AEG using negative enrichment-fluorescence in situ hybridization technology

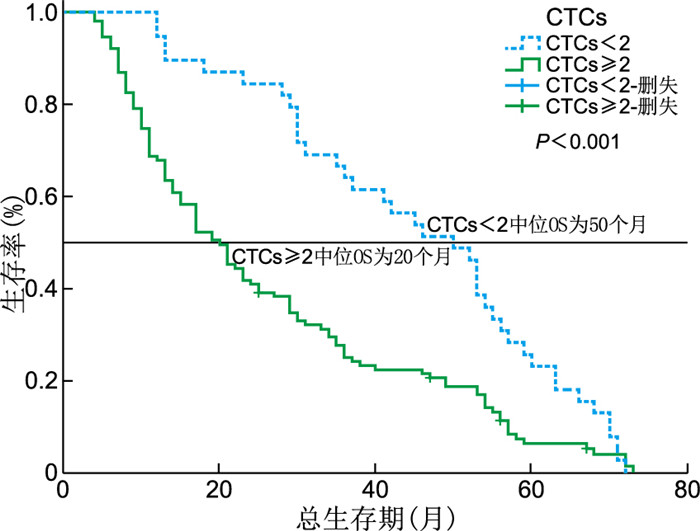
图 2 CTCs≥2与CTCs < 2的AEG患者OS生存曲线
Figure 2. OS survival curves of AEG patients with CTCs≥2 and CTCs < 2

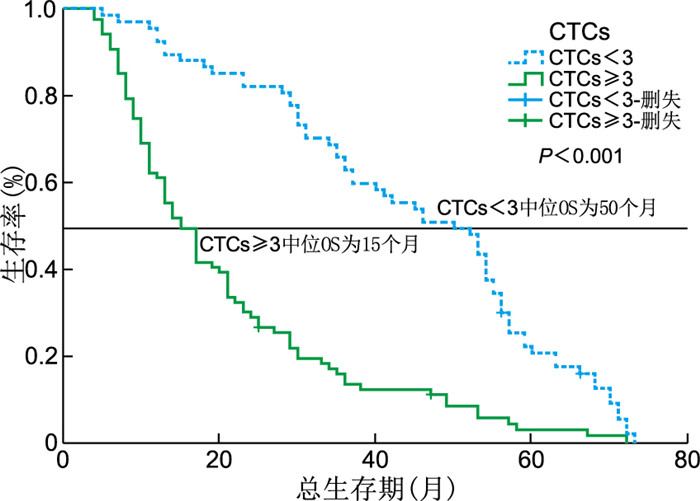
图 3 CTCs≥3与CTCs < 3的AEG患者OS生存曲线
Figure 3. OS survival curves of AEG patients with CTCs≥3 and CTCs < 3
表 1 不同CTCs计数AEG患者临床特征比较[例(%)]
Table 1. Comparison of clinical features in AEG patients with different CTCs counts [cases (%)]
项目 例数 CTCs计数 χ2值 P值 < 2 ≥2 性别 2.156 0.142 男性 131 36(27.5) 95 (72.5) 女性 23 3 (13.0) 20 (87.0) 年龄(岁) 1.257 0.262 < 65 59 12 (20.3) 47 (79.7) ≥65 95 27 (28.4) 68 (71.6) 肿瘤分化程度 4.958 0.026 高分化 14 7 (50.0) 7 (50.0) 中低分化 140 32 (22.9) 108(77.1) 脉管内癌栓 45.262 < 0.001 无 54 31 (57.4) 23 (42.6) 有 100 8 (8.0) 92 (92.0) T分期 9.082 0.003 T1+T2 36 16 (44.4) 20 (55.6) T3+T4 118 23 (19.5) 95 (80.5) 淋巴结转移 5.158 0.023 无 35 14 (40.0) 21 (60.0) 有 119 25 (21.0) 94 (79.0) TNM分期 14.304 < 0.001 Ⅰ~Ⅱ期 56 24 (42.9) 32 (57.1) Ⅲ~Ⅳ期 98 15 (15.3) 83 (84.7) CEA(ng/mL) 1.781 0.182 < 5 101 29 (28.7) 72 (71.3) ≥5 53 10 (18.9) 43 (81.1) CA19-9(U/mL) 2.177 0.140 < 39 136 37 (27.2) 99 (72.8) ≥39 18 2 (11.1) 16 (88.9) CA72-4(U/mL) 0.464 0.540 < 6.9 112 30 (26.8) 82 (73.2) ≥6.9 42 9 (21.4) 33 (78.6)  下载: 导出CSV
下载: 导出CSV
表 2 不同临床特征AEG患者中位OS比较
Table 2. Comparison of median OS in AEG patients with different clinical characteristics
项目 例数 中位OS(95% CI,月) χ2值 P值 性别 0.502 0.479 男性 131 27.00(21.11~32.89) 女性 23 29.00(16.57~41.43) 年龄(岁) 0.987 0.321 < 65 59 30.00(19.26~40.74) ≥65 95 24.00(18.66~29.34) 肿瘤分化程度 0.310 0.578 高分化 14 36.00(23.30~48.70) 中低分化 140 24.00(18.23~29.77) CTCs 12.486 < 0.001 < 2 39 50.00(40.39~59.61) ≥2 115 20.00(15.40~24.59) CTCs 45.344 < 0.001 < 3 67 50.00(38.97~61.03) ≥3 87 15.00(11.95~18.05) 脉管内癌栓 29.318 < 0.001 有 100 17.00(12.11~21.89) 无 54 49.00(41.80~56.20) T分期 1.285 0.257 T1+T2 36 36.00(22.79~49.21) T3+T4 118 21.00(16.09~25.91) 淋巴结转移 12.299 < 0.001 有 35 21.00(16.51~25.49) 无 119 52.00(45.48~58.52) TNM分期 17.627 < 0.001 Ⅰ~Ⅱ 56 49.00(40.62~57.38) Ⅲ~Ⅳ 98 17.00(12.15~21.85) CEA(ng/mL) 10.837 0.001 < 5 101 33.00(27.26~38.75) ≥5 53 13.00(9.94~16.06) CA19-9(U/mL) 27.934 < 0.001 < 39 136 30.00(25.48~34.52) ≥39 18 10.00(7.93~12.07) CA72-4(U/mL) 14.371 < 0.001 < 6.9 112 31.00(25.88~36.12) ≥6.9 42 13.00(9.49~16.51)
下载: 导出CSV
表 3 AEG患者OS影响因素的Cox多因素回归分析
Table 3. Cox multivariate regression analysis of factors influencing OS in AEG patients
变量 B SE Waldχ2 P值 HR值(95%CI) 性别(男性vs. 女性) 0.173 0.263 0.434 0.510 1.189(0.711~1.989) 年龄(< 65岁vs. ≥65岁) 0.108 0.192 0.315 0.575 1.114(0.764~1.623) CTCs(< 2 vs. ≥2) 0.123 0.281 0.190 0.663 1.130(0.651~1.962) CTCs(< 3 vs. ≥3) 0.900 0.262 11.806 0.001 2.459(1.472~4.107) 分化程度(高vs. 中低) -0.198 0.365 0.294 0.588 0.820(0.401~1.678) T分期(T1+T2 vs. T3+T4) -0.513 0.322 2.535 0.111 0.599(0.318~1.126) 淋巴结转移(有vs. 无) -0.015 0.324 0.002 0.964 0.986(0.522~1.861) TNM分期(Ⅰ~Ⅱ vs. Ⅲ~Ⅳ) 0.511 0.386 1.758 0.185 1.668(0.783~3.552) 脉管内瘤栓(无vs. 有) 0.229 0.255 0.807 0.369 1.257(0.763~2.071) CEA(< 5 ng/mL vs. ≥5 ng/mL) -0.084 0.212 0.155 0.694 0.920(0.607~1.395) CA19-9(< 39 U/mL vs. ≥39 U/mL) 0.704 0.290 5.882 0.015 2.022(1.145~3.572) CA72-4(< 6.9 U/mL vs. ≥6.9 U/mL) 0.458 0.234 3.830 0.050 1.580(0.999~2.499) 注:变量赋值方法如下,性别(男性=0,女性=1),年龄(< 65岁=0,≥65岁=1),CTCs(< 2=0,≥2=1),CTCs(< 3=0,≥3=1),分化程度(高=0,中低=1),T分期(T1+T2=0,T3+T4=1),淋巴结转移(有=1,无=0),TNM分期(Ⅰ+Ⅱ=0,Ⅲ+Ⅳ=1),脉管内瘤栓(无=0,有=1),CEA(< 5 ng/mL=0,≥5 ng/mL=1),CA19-9(< 39 U/mL=0,≥39 U/mL=1),CA72-4(< 6.9 U/mL=0,≥6.9 U/mL=1)。
下载: 导出CSV
-
[1] SUNG H, FERLAY J, SIEGEL R L, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. Ca Cancer J Clin, 2021, 71(3): 209-249. doi: 10.3322/caac.21660 [2] WANG H L, ZHAO X K, ZHOU F Y, et al. Characterization of e-cadherin expression in normal mucosa, dysplasia and adenocarcinoma of gastric cardia and its influence on prognosis[J]. World J Gastrointest Oncol, 2022, 14(1): 265-277. doi: 10.4251/wjgo.v14.i1.265 [3] LI Y, MA G, ZHAO P, et al. Improvement of sensitive and specific detection of circulating tumor cells using negative enrichment and immunostaining-fish[J]. Clin Chim Acta, 2018, 485(1): 95-102. [4] MA G, YANG D, LI Y, et al. Combined measurement of circulating tumor cell counts and serum tumor marker levels enhances the screening efficiency for malignant versus benign pulmonary nodules[J]. Thorac Cancer, 2022, 13(23): 3393-3401. doi: 10.1111/1759-7714.14702 [5] LI Y, WANG Z, FU R, et al. Clinical utility of circulating tumor cells in patients with esophageal cancer[J]. Front Oncol, 2022, 12(2): 60-68. [6] JELSKI W, MROCZKO B. Molecular and circulating biomarkers of gastric cancer[J]. Int J Mol Sci, 2022, 23(14): 75-88. [7] MA S, ZHOU M, XU Y, et al. Clinical application and detection techniques of liquid biopsy in gastric cancer[J]. Mol Cancer, 2023, 22(1): 7. doi: 10.1186/s12943-023-01715-z [8] XU J, LIAO K, YANG X, et al. Using single-cell sequencing technology to detect circulating tumor cells in solid tumors[J]. Mol Cancer, 2021, 20(1): 96-104. doi: 10.1186/s12943-021-01388-6 [9] GALVIS M M, ROMERO C S, BUENO T O, et al. Toward a new era for the management of circulating tumor cells[J]. Adv Exp Med Biol, 2021, 1286(3): 125-134. [10] MA X, OU K, LIU X, et al. Application progress of liquid biopsy in gastric cancer[J]. Front Oncol, 2022, 12(10): 54-66. [11] GKOUNTELA S, CASTRO-GINER F, SZCZERBA B M, et al. Circulating tumor cell clustering shapes DNA methylation to enable metastasis seeding[J]. Cell, 2019, 176(2): 98-112. [12] CHENG B, TONG G, WU X, et al. Enumeration and characterization of circulating tumor cells and its application in advanced gastric cancer[J]. Onco Targets Ther, 2019, 12(6): 7887-7896. [13] JHI J H, KIM G H, PARK S J, et al. Circulating tumor cells and twist expression in patients with metastatic gastric cancer: a preliminary study[J]. J Clin Med, 2021, 10(19): 70-81. [14] YANG Y, ZHENG J, LI Y. Comparison of 4 lymph node staging systems for the prognostic prediction of esophagogastric junction adenocarcinoma with ≤ 15 retrieved lymph nodes[J]. Eur J Surg Oncol, 2022, 48(5): 1017-1024. doi: 10.1016/j.ejso.2021.11.133 [15] ZENG C D D, JIN C C, GAO C, et al. Preoperative folate receptor-positive circulating tumor cells are associated with occult peritoneal metastasis and early recurrence in gastric cancer patients: a prospective cohort study[J]. Front Oncol, 2022, 29(12): 191-203. [16] 赵天豪, 杨一群, 李岳彤, 等. 泛素结合酶2S在胃癌中的表达及临床意义[J]. 中华全科医学, 2023, 21(4): 555-559. doi: 10.16766/j.cnki.issn.1674-4152.002929ZHAO T H, YANG Y Q, LI Y T, et al. Expression and clinical significance of UBE2S in gastric cancer[J]. Chinese Journal of General Practice, 2023, 21(4): 555-559. doi: 10.16766/j.cnki.issn.1674-4152.002929 [17] SONG X H, LIU K, YANG S J, et al. Prognostic value of changes in preoperative and postoperative serum CA19-9 levels in gastric cancer[J]. Front Oncol, 2020, 10(2): 22-32. [18] WANG Y W, LI L L, LU M, et al. Stem cell-like circulating tumor cells indicate poor prognosis in gastric cancer[J]. Arch Med Sci, 2022, 18(5): 1297-1307. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 702
- HTML全文浏览量: 427
- PDF下载量: 4
- 被引次数: 0
