

The clinical value of IL-6 in predicting the incidence of pulmonary infections during chemotherapy period in patients with multiple myeloma
-
摘要:
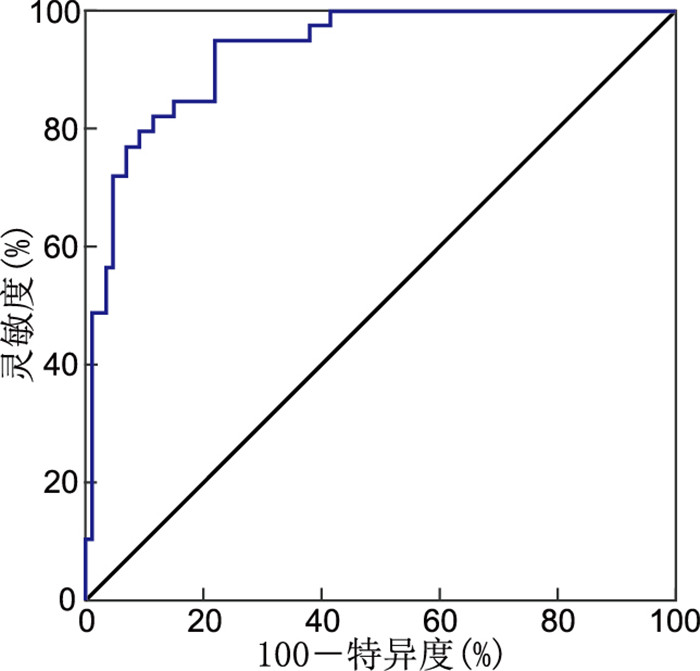
目的 探讨多发性骨髓瘤(MM)患者血清中IL-6表达与肺部感染的相关性。 方法 纳入2021年1月—2022年8月就诊于新乡医学院第一附属医院血液内科的160例MM患者(MM组)和40例健康体检者(对照组)作为研究对象。根据MM患者化疗期间是否发生肺部感染分为感染组(65例)和未感染组(95例),并对肺部感染患者呼吸道分泌物进行细菌培养和鉴定。分析MM患者化疗期间发生肺部感染的危险因素,采用ROC曲线分析血清中IL-6表达水平预测MM患者化疗期间发生肺部感染的临床效能。 结果 与对照组比较,MM组血清中IL-6表达水平升高[(76.45±6.59)mg/mL vs. (34.23±4.34)mg/mL,t=38.449,P < 0.001]。感染组分泌物中共检测出78株病原菌,其中革兰阳性菌占52.56%(41/78),革兰阴性菌占43.59%(34/78),真菌占3.85%(3/78)。Durie-Salmon分期、国际标准分期、合并粒细胞缺乏症和IL-6均为MM患者化疗期间发生肺部感染的影响因素。血清中IL-6预测MM患者化疗期间发生肺部感染的AUC为0.924,诊断灵敏度和特异度分别为89.35%和93.22%。 结论 MM患者血清中IL-6表达水平升高,化疗前血清中IL-6可作为预测MM患者化疗期间发生肺部感染的一项血清学标志物。 Abstract:Objective This study aims to investigate the correlation between serum IL-6 expression levels and the occurrence of pulmonary infection in patients with multiple myeloma (MM). Methods This study enrolled a total of 160 MM patients diagnosed with multiple myeloma (MM group) and 40 healthy controls (Control group) from the Department of Hematology of the First Affiliated Hospital of Xinxiang Medical University between January 2021 and August 2022. Within the MM group, patients were divided into an infected group (n=65) and an uninfected group (n=95) according to the incidence of pulmonary infection during chemotherapy. Respiratory secretions were subjected to bacterial culture and identification. Risk factors of pulmonary infection in MM patients during chemotherapy period was analyzed. The clinical value of serum IL-6 expression levels in predicting the incidence of pulmonary infection during chemotherapy in MM patients was assessed using ROC curve analysis. Results Compared to the control group, the serum IL-6 expression level in the MM group significantly increased [(76.45±6.59) mg/mL vs. (34.23±4.34) mg/mL, t=38.449, P < 0.001]. Among the infected group, a total of 78 strains of pathogenic bacteria were detected, with gram-positive bacteria accounting for 52.56% (41/78), gram-negative bacteria accounting for 43.59% (34/78), and fungi accounting for 3.85% (3/78). Logistic regression analysis showed that Durie-Salmon stage, international staging system stage, agranulocytosis, and IL-6 were identified as influence factors for pulmonary infection during the chemotherapy period in MM patients. The area under the curve for serum IL-6 in predicting pulmonary infection during chemotherapy in MM patients was 0.924. The diagnostic sensitivity and specificity were 89.35% and 93.22%, respectively. Conclusion The serum expression level of IL-6 is significantly increased in MM patients. The pre-chemotherapy serum IL-6 expression level in MM patients can be used as a serological marker to predict the incidence of pulmonary infection during their chemotherapy period. -
Key words:
- Multiple myeloma /
- Pulmonary infection /
- IL-6 /
- Sensitivity /
- Specificity /
- Marker
-

图 1 IL-6预测MM患者化疗期间发生肺部感染的ROC曲线
Figure 1. ROC curve of IL-6 predicting pulmonary infection occurrence during chemotherapy in MM patients
表 1 78例肺部感染患者致病菌株分布情况
Table 1. Pathogenic strain distribution among 78 patients with pulmonary infections
病原菌 菌株数量 构成比(%) 革兰阳性菌株 41 52.56 金黄色葡萄球菌 21 26.92 溶血葡萄球菌 13 16.67 肺炎链球菌 7 8.97 革兰阴性菌株 34 43.59 铜绿假单胞菌 15 19.23 肺炎克雷伯菌 13 16.67 大肠埃希菌 4 5.13 鲍氏不动杆菌 2 2.56 真菌 3 3.85 酵母菌 3 3.85  下载: 导出CSV
下载: 导出CSV
表 2 2组MM患者临床资料比较
Table 2. Comparison of clinical data between two groups of MM patients
项目 未感染组(n=95) 感染组(n=65) 统计量 P值 性别(男/女, 例) 55/40 35/30 0.257a 0.612 年龄(x±s, 岁) 60.35±4.98 61.74±5.02 1.728b 0.086 吸烟史[例(%)] 2.093a 0.148 有 32(33.68) 15(23.08) 无 63(66.32) 50(76.92) 饮酒史[例(%)] 1.459a 0.227 有 27(28.42) 13(20.00) 无 68(71.58) 52(80.00) BMI(x±s) 27.54±5.23 26.93±4.78 0.750b 0.454 DS分期[例(%)] 4.944a 0.026 Ⅰ~Ⅱ期 55(57.89) 26(40.00) Ⅲ期 40(42.10) 39(60.00) ISS分期[例(%)] 8.222a 0.004 Ⅰ~Ⅱ期 57(60.00) 24(36.92) Ⅲ期 38(40.00) 41(63.08) EOCG评分[例(%)] 10.512a 0.001 0~2分 68(71.58) 30(46.15) >2分 27(28.42) 35(53.85) 合并粒细胞缺乏症[例(%)] 37(38.95) 41(63.08) 8.993a 0.003 WBC(x±s, ×109/L) 8.45±1.36 8.68±1.27 1.079b 0.282 N(x±s, ×109/L) 3.47±0.18 3.52±0.27 1.406b 0.162 hs-CRP(x±s, mg/L) 7.26±1.27 6.96±1.31 1.449b 0.149 ESR(x±s, mm/h) 18.67±3.21 17.98±4.34 1.156b 0.250 PCT(x±s, mg/L) 0.43±0.12 0.45±0.11 0.535b 0.593 白蛋白(x±s, g/L) 43.93±5.60 45.01±5.43 1.213b 0.227 IL-6(x±s, mg/mL) 69.78±6.37 82.07±7.55 11.110b < 0.001 注:a为χ2值,b为t值。
下载: 导出CSV
表 3 变量赋值情况
Table 3. Variable assignment
变量 赋值方法 发生肺部感染 有=1,无=0 性别 男性=1,女性=0 年龄 以实际值赋值 吸烟史 有=1,无=0 饮酒史 有=1,无=0 BMI 以实际值赋值 DS分期 Ⅲ期=1,Ⅰ~Ⅱ期=0 ISS分期 Ⅲ期=1,Ⅰ~Ⅱ期=0 EOCG评分 >2分=1,0~2分=0 合并粒细胞缺乏症 有=1,无=0 WBC 以实际值赋值 N 以实际值赋值 hs-CRP 以实际值赋值 ESR 以实际值赋值 PCT 以实际值赋值 白蛋白 以实际值赋值 IL-6 以实际值赋值
下载: 导出CSV
表 4 MM患者化疗期间发生肺部感染影响因素的logistic回归分析
Table 4. Logistic regression analysis of factors influencing pulmonary infection in multiple myeloma patients during chemotherapy
变量 B SE Waldχ2 P值 OR(95% CI) DS分期(Ⅲ期) 0.982 0.574 2.929 < 0.001 2.671(1.222~5.021) ISS分期(Ⅲ期) 0.869 0.595 2.134 < 0.001 2.385(1.175~6.773) 合并粒细胞缺乏症 0.628 0.485 1.674 0.016 1.873(1.214~4.058) IL-6 1.104 0.789 1.956 < 0.001 3.015(1.269~6.127)
下载: 导出CSV
-
[1] 李志超, 黄方, 郝思国. 多发性骨髓瘤免疫治疗研究进展[J]. 安徽医学, 2023, 44(4): 363-366. doi: 10.3969/j.issn.1000-0399.2023.04.001 [2] CAO W, CHEN H D, YU Y W, et al. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020[J]. Chin Med J(Engl), 2021, 134(7): 783-791. [3] 刘淑艳, 张蕴, 林圣云. 基于PI3K/AKT/mTOR探索硼替佐米对多发性骨髓瘤侧群细胞的作用机制[J]. 中华全科医学, 2020, 18(3): 365-369. doi: 10.16766/j.cnki.issn.1674-4152.001248 [4] 张天琰, 阳梅, 吴秋慧, 等. 含硼替佐米化疗的两种方案治疗初治多发性骨髓瘤疗效及对患者总生存期和毒副反应的影响[J]. 实用医院临床杂志, 2020, 17(2): 242-245. doi: 10.3969/j.issn.1672-6170.2020.02.071 [5] 陆亚军, 南萍, 龚富婷, 等. 血清β2-MG联合PCT预测多发性骨髓瘤化疗患者肺部感染的价值[J]. 中国国境卫生检疫杂志, 2023, 46(2): 183-187. [6] 张新芸, 华冰清, 高山, 等. 多发性骨髓瘤化疗医院感染风险预测模型的建立及应用价值[J]. 中华医院感染学杂志, 2021, 31(9): 1396-1400. [7] 韩少玲, 吴亚兵, 张家友, 等. 多发性骨髓瘤患者血清β2-MG、CRP和IL-6水平与临床分期的关系[J]. 河北医药, 2021, 43(3): 353-356. [8] 中国医师协会血液科医师分会, 中华医学会血液学分会. 中国多发性骨髓瘤诊治指南(2022年修订)[J]. 中华内科杂志, 2022, 61(5): 480-487. [9] 千晨静, 洪梅, 夏凌辉. 多发性骨髓瘤新型治疗方案的研究进展[J]. 肿瘤防治研究, 2023, 50(3): 321-325. https://www.cnki.com.cn/Article/CJFDTOTAL-ZLFY202303011.htm [10] 毛沛沛, 杨琛. 硼替佐米联合地塞米松、来那度胺化疗方案治疗多发性骨髓瘤的疗效和安全性评价[J]. 实用癌症杂志, 2023, 38(3): 502-506. https://www.cnki.com.cn/Article/CJFDTOTAL-SYAZ202303039.htm [11] AKHMETZYANOVA I, AARON T, GALBO P, et al. Tissue-resident macrophages promote early dissemination of multiple myeloma via IL-6 and TNF-α[J]. Blood Adv, 2021, 5(18): 3592-3608. [12] XU L, YAO Y, LU T, et al. miR-451a targeting IL-6R activates JAK2/STAT3 pathway, thus regulates proliferation and apoptosis of multiple myeloma cells[J]. J Musculoskelet Neuronal Interact, 2022, 22(2): 251-260. [13] 杨蔓玲, 王莉丽, 侯儆, 等. 促红细胞生成素、白细胞介素-6与C-反应蛋白在血液透析治疗多发性骨髓瘤患者中的变化及预测价值研究[J]. 标记免疫分析与临床, 2023, 30(3): 445-451. [14] 张丽红, 王宣, 尹婉宜, 等. 多发性骨髓瘤患者骨髓单个核细胞Treg、Th17和血清IL-6、IL-10与临床分期以及治疗效果的关系分析[J]. 现代生物医学进展, 2022, 22(14): 2713-2717. [15] BRIGHTON T A, KHOT A, HARRISON S J, et al. Randomized, double-blind, placebo-controlled, multicenter study of siltuximab in high-risk smoldering multiple myeloma[J]. Clin Cancer Res, 2019, 25(13): 3772-3775. [16] 刘莹, 隋靖喆, 朱丽华, 等. IL-6通过STAT3/Notch信号通路调控多发性骨髓瘤耐药细胞株对硼替佐米的化疗敏感性[J]. 中国实验血液学杂志, 2022, 30(5): 1474-1481. [17] 任韩雯婧, 张川, 乐涛, 等. ICU重症肺部感染患者血清IL-6、IL-1β、IL-8和TNF-α水平变化及其与预后的关系[J]. 热带医学杂志, 2022, 22(10): 1371-1375, 1390. [18] 任静静, 杨瑜, 王珊珊. 血清乳酸脱氢酶、β2-微球蛋白水平与多发性骨髓瘤患者预后的关系[J]. 癌症进展, 2023, 21(12): 1337-1340. https://www.cnki.com.cn/Article/CJFDTOTAL-AZJZ202312010.htm [19] 王紫宁, 陈浩然, 张钧栋, 等. 多发性骨髓瘤铁死亡相关组学分析及预后模型的建立[J]. 中国实验血液学杂志, 2023.31(2): 411-419. https://www.cnki.com.cn/Article/CJFDTOTAL-XYSY202302015.htm [20] 赵佳莉, 饶琦, 罗茜. 老年初治多发性骨髓瘤化疗后感染临床特点及预后的多因素分析[J]. 老年医学与保健, 2021, 27(4): 758-762. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 910
- HTML全文浏览量: 657
- PDF下载量: 10
- 被引次数: 0
