

Value of c-MYC expression in a lymph node metastasis risk prediction model for colon cancer
-
摘要:
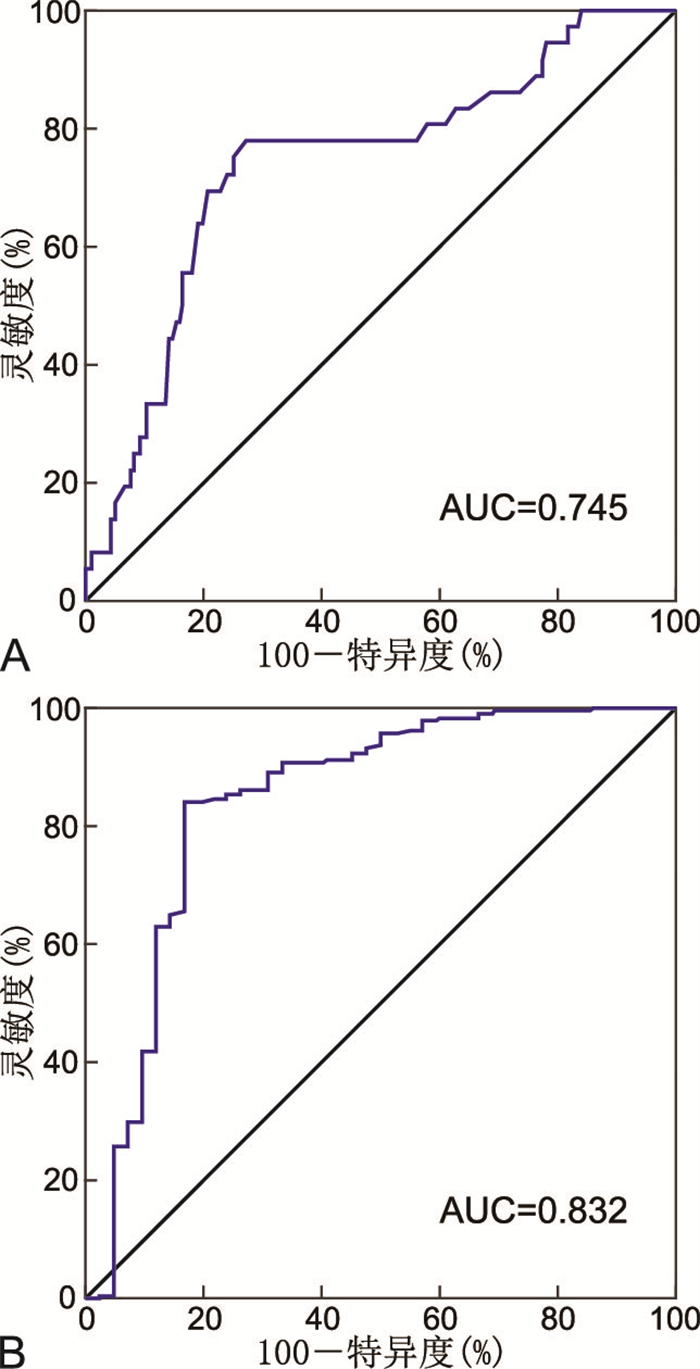
目的 研究细胞-骨髓细胞瘤病病毒癌基因(c-MYC)表达等病理因素与结肠癌淋巴结转移风险的相关性,构建风险预测模型,评估其预测价值。 方法 收集2020年1月—2022年12月于蚌埠医科大学第一附属医院行结肠癌根治术的304例患者的病历资料,将所有患者按分层随机法分为模型组和验证组,各152例。分析淋巴结转移的影响因素,确定淋巴结转移的风险变量,作为预测模型输入节点,通过人工智能系统深度学习后分析结肠癌淋巴结转移的特点,并检测模型的有效性。 结果 单因素分析显示,不同中性粒细胞与淋巴细胞比值、c-MYC、肿瘤形态、脉管癌栓、肿瘤长径、肿瘤分化程度结肠癌患者的淋巴结转移率差异有统计学意义。进一步行多因素分析发现,中性粒细胞与淋巴细胞比值、c-MYC、肿瘤形态、脉管癌栓、肿瘤长径、肿瘤分化程度是影响结肠癌淋巴结转移的相关风险变量。根据预测模型绘制ROC曲线,结果显示,验证组的AUC为0.745(95% CI:0.712~0.803),模型组的AUC为0.832(95% CI:0.796~0.875),提示风险预测模型能有效预测结肠癌患者的淋巴结转移风险。 结论 中性粒细胞与淋巴细胞比值、c-MYC、肿瘤形态、脉管癌栓、肿瘤长径、肿瘤分化程度是影响结肠癌淋巴结转移的相关风险变量。本研究构建的风险预测模型能够较为准确地识别出结肠癌患者的淋巴结转移风险,具有临床应用前景。 -
关键词:
- 结肠癌 /
- 淋巴结转移 /
- 细胞-骨髓细胞瘤病病毒癌基因 /
- 预测模型
Abstract:Objective To examine the correlation between the expression of cellular-myelocytomatosis viral oncogene (c-MYC) and lymph node metastasis risk in colon cancer, develop a risk prediction model and evaluate its significance. Methods The medical records of 304 patients who underwent radical colon cancer surgery at the First Affiliated Hospital of Bengbu Medical University from January 2020 to December 2022 were collected. The patients were randomly divided into a model group and a validation group, each comprising 152 cases. We analyzed the factors influencing lymph node metastasis and identified the risk variables for input into the prediction model. The characteristics of colon cancer lymph node metastasis were then analyzed using an artificial intelligence system through deep learning. Finally, we assessed the effectiveness of the model. Results Univariate analysis showed that the neutrophil-to-lymphocyte ratio (NLR), c-MYC expression, tumor morphology, vascular cancer thrombus, tumor length, and tumor differentiation degree of 152 colon cancer patients in the model group were related to their lymph node metastasis. Further multivariate analysis identified the neutrophil-lymphocyte ratio, c-MYC expression, tumor morphology, vascular cancer thrombus, tumor length and diameter, and tumor differentiation degree as significant risk relevant variables for lymph node metastasis in colon cancer. The ROC curve based on the prediction model showed an AUC of 0.745 (95% CI: 0.712-0.803) in the validation group and 0.832 (95% CI: 0.796-0.875) in the model group, suggesting the effective predictive capability of the risk prediction model for lymph node metastasis in colon cancer patients. Conclusion The NLR, c-MYC expression, tumor morphology, vascular cancer thrombus, tumor length, and tumor differentiation were significant risk variables affecting lymph node metastasis in colon cancer. The risk prediction model constructed in this study demonstrates accurate identification of lymph node metastasis risk in colon cancer patients, holding promising clinical applications. -

图 1 c-MYC在结肠癌细胞中的表达情况(免疫组化染色,×40)
注:Ⅰ级,阳性细胞数为5%~10%;Ⅱ级,阳性细胞数为11%~20%;Ⅲ级,阳性细胞数为21%~30%;Ⅳ级,阳性细胞数>30%。
Figure 1. Expression of c-MYC in colon cancer cells (immunohistochemical staining, ×40)

图 2 结肠癌患者淋巴结转移风险预测模型特异性
注:A为验证组,B为模型组。
Figure 2. Specificity of the risk prediction model for lymph node metastasis in colon cancer patients

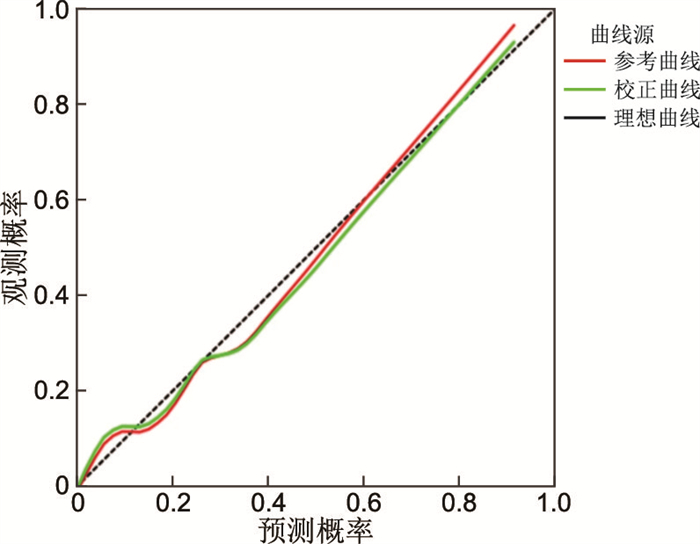
图 3 结肠癌患者淋巴结转移风险预测模型预测概率
Figure 3. Prediction probability of the risk prediction model for lymph node metastasis in colon cancer patients
表 1 模型组与验证组结肠癌患者临床病理特征比较[例(%)]
Table 1. Comparison of clinicopathological characteristics of colon cancer patients between the model group and the validation group [cases (%)]
项目 模型组(n=152) 验证组(n=152) χ2值 P值 性别 1.802a 0.097 男性 107(70.4) 114(75.0) 女性 45(29.6) 38(25.0) 年龄(岁) 0.144a 0.268 <55 82(53.9) 69(45.4) ≥55 70(46.1) 83(54.6) c-MYC 1.630a 0.276 低表达 60(39.5) 71(46.7) 高表达 92(60.5) 81(53.3) CEA 0.063a 0.141 正常 61(40.1) 66(43.4) 升高 91(59.9) 86(56.6) 肿瘤部位 41.384a 0.063 左半结肠 22(14.5) 25(16.4) 横结肠 43(28.3) 41(27.0) 右半结肠 21(13.8) 38(25.0) 乙状结肠 66(43.4) 48(31.6) 肿瘤形态 6.074a 0.391 肿块型 37(24.4) 32(21.1) 溃疡型 59(38.8) 55(36.2) 浸润型 56(36.8) 65(42.7) 淋巴结转移 2.129a 0.105 有 92(60.5) 100(65.8) 无 60(39.5) 52(34.2) 脉管癌栓 1.621a 0.061 有 70(46.1) 73(48.0) 无 82(53.9) 79(52.0) 肿瘤长径(cm) 0.192a 0.349 <2 63(41.4) 53(34.9) ≥2 89(58.6) 99(65.1) NLR 0.462b 0.720 低 50(32.9) 44(28.9) 中 61(40.1) 55(36.2) 高 41(27.0) 53(34.9) 分化程度 0.787b 0.432 高 20(13.2) 28(18.4) 中 62(40.8) 59(38.8) 低 70(46.1) 65(42.8) 肿瘤分期(TNM分期) 0.276b 0.111 Ⅰ期 20(13.2) 15(9.9) Ⅱ期 40(26.3) 37(24.3) Ⅲ期 82(53.9) 92(60.5) Ⅳ期 10(6.6) 8(5.3) 注:a为χ2值,b为Z值。  下载: 导出CSV
下载: 导出CSV
表 2 模型组结肠癌患者淋巴结转移的单因素分析
Table 2. Univariate analysis of lymph node metastasis in colon cancer patients in the model group
项目 例数 淋巴结转移[例(%)] χ2值 P值 性别 0.416a 0.138 男性 107 70(65.4) 女性 45 22(48.9) 年龄(岁) 2.027a 0.354 <55 82 57(69.5) ≥55 70 35(50.0) NLR 4.622b 0.026 低 50 31(62.0) 中 61 34(55.7) 高 41 27(65.9) c-MYC 1.279a 0.025 低表达 60 31(51.7) 高表达 92 61(66.3) CEA 1.382a 0.602 正常 61 36(59.0) 升高 91 56(61.5) 肿瘤部位 28.025a 0.083 左半结肠 22 12(54.5) 横结肠 43 27(62.8) 右半结肠 21 13(61.9) 乙状结肠 66 40(60.6) 肿瘤形态 2.487a 0.003 肿块型 37 12(32.4) 溃疡型 59 45(76.3) 浸润型 56 35(62.5) 脉管癌栓 6.483a 0.006 有 70 50(71.4) 无 82 42(51.2) 肿瘤长径(cm) 4.705a 0.029 <2 63 39(61.9) ≥2 89 53(59.6) 分化程度 0.924b 0.008 高 20 9(45.0) 中 62 40(64.5) 低 70 43(61.4) 肿瘤分期(TNM分期) - - Ⅰ期 20 0 Ⅱ期 40 0 Ⅲ期 82 82(100.0) Ⅳ期 10 10(100.0) 注:a为χ2值,b为Z值。“-”为未比较。
下载: 导出CSV
表 3 模型组结肠癌患者淋巴结转移的多因素分析
Table 3. Multivariate analysis of lymph node metastasis in colon cancer patients in the model group
变量 B SE Waldχ2 P值 OR值 95% CI NLR 0.359 0.125 8.382 0.007 1.432 1.123~1.531 c-MYC 1.005 0.329 9.316 < 0.001 2.733 1.433~5.212 肿瘤形态 0.294 0.134 4.818 0.028 1.342 1.032~1.433 脉管癌栓 1.084 0.517 5.745 0.032 2.955 1.103~7.924 肿瘤长径 1.087 0.504 4.531 0.031 2.965 1.095~8.013 分化程度 0.185 0.078 5.582 0.017 1.203 1.032~1.433 注:变量赋值如下,NLR(低=1,中=2,高=3);MYC(低=0,高=1);肿瘤形态(肿块型为0, 0;溃疡型为0, 1;浸润型为1, 0);肿瘤癌栓(无=0,有=1);肿瘤长径(<2 cm=0,≥2 cm=1);分化程度(高=1,中=2,低=3)。
下载: 导出CSV
-
[1] DHANASEKARAN R, DEUTZMANN A, MAHAUAD W D, et al. The MYC oncogene: the grand orchestrator of cancer growth and immune evasion[J]. Nat Rev Clin Oncol, 2022, 19(1): 23-36. doi: 10.1038/s41571-021-00549-2 [2] CHUANG J P, TSAI H L, CHEN P J, et al. Comprehensive review of biomarkers for the treatment of locally advanced colon cancer[J]. Cells, 2022, 11(23): 37-44. [3] DUFFY M J, GRADY S, TANG M, et al. MYC as a target for cancer treatment[J]. Cancer Treat Rev, 2021, 94(2): 152-154. [4] TANG J, YAN T, BAO Y, et al. LncRNA GLCC1 promotes colorectal carcinogenesis and glucose metabolism by stabilizing c-Myc[J]. Nat Commun, 2019, 10(1): 34-39. doi: 10.1038/s41467-018-08006-y [5] GEORGE J, LI Y, KADAMBERI I P, et al. RNA-binding protein FXR1 drives cMYC translation by recruiting eIF4F complex to the translation start site[J]. Cell Rep, 2021, 37(5): 109-114. [6] SINGH K B, HAHM E R, SINGH S V. Leelamine suppresses cMYC expression in prostate cancer cells in vitro and inhibits prostate carcinogenesis in vivo[J]. J Cancer Metastasis Treat, 2021, 7(16): 704-722. [7] MIHASHI Y, KIMURA S, IWASAKI H, et al. Large cell morphology, CMYC+ tumour cells, and PD-1+ tumour cell/intense PD-L1+ cell reactions are important prognostic factors in nodal peripheral T-cell lymphomas with T follicular helper markers[J]. Diagn Pathol, 2021, 16(1): 101-105. doi: 10.1186/s13000-021-01163-7 [8] WU H, YANG T Y, LI Y, et al. Tumor necrosis factor receptor-associated factor 6 promotes hepatocarcinogenesis by interacting with histone deacetylase 3 to enhance c-Myc gene expression and protein stability[J]. Hepatology, 2020, 71(1): 148-163. doi: 10.1002/hep.30801 [9] ROBISON T H, SOLIPURAM M, HEIST K, et al. Multiparametric MRI to quantify disease and treatment response in mice with myeloproliferative neoplasms[J]. JCI Insight, 2022, 7(19): 161-167. [10] MIN J K, KWAK M S, CHA J M. Overview of deep learning in gastrointestinal endoscopy[J]. Gut Liver, 2019, 13(4): 388-393. doi: 10.5009/gnl18384 [11] LI K, FATHAN M I, PATEL K, et al. Colonoscopy polyp detection and classification: dataset creation and comparative evaluations[J]. PLoS One, 2021, 16(8): 254-259. [12] BLANES V, BAATRUP G, NADIMI E S. Addressing priority challenges in the detection and assessment of colorectal polyps from capsule endoscopy and colonoscopy in colorectal cancer screening using machine learning[J]. Acta Oncol, 2019, 58(sup1): S29-S36. doi: 10.1080/0284186X.2019.1584404 [13] SHINJI S, YAMADA T, MATSUDA A, et al. Recent advances in the treatment of colorectal cancer: a review[J]. Nippon Med Sch, 2022, 89(3): 246-254. doi: 10.1272/jnms.JNMS.2022_89-310 [14] YANG C Y, YEN M H, KIU K T, et al. Outcomes of right-sided and left-sided colon cancer after curative resection[J]. Sci Rep, 2022, 12(1): 118-123. doi: 10.1038/s41598-021-02808-9 [15] 柳亚魁, 王栓虎. Ⅰ~Ⅲ期不同部位的左右半结肠癌临床病理特征及预后比较分析[J]. 中华全科医学, 2022, 20(4): 587-590. doi: 10.16766/j.cnki.issn.1674-4152.002406LIU Y K, WANG S H. Comparative analysis on the clinicopathological characteristics and prognosis of left and right colon cancer at stageⅠ-Ⅲ[J]. Chinese Journal of General Practice, 2022, 20(4): 587-590. doi: 10.16766/j.cnki.issn.1674-4152.002406 [16] JIN J, ZHANG Q, DONG B, et al. Automatic detection of early gastric cancer in endoscopy based on Mask region-based convolutional neural networks (Mask R-CNN) (with video)[J]. Front Oncol, 2022, 12(9): 278-288. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 863
- HTML全文浏览量: 407
- PDF下载量: 10
- 被引次数: 0
